
User:ScotXW/Dietary fiber
The dietary fibers or roughage are the indigestible portion of food. For a long time, dietary fiber has been regarded as irksome to digestion and therefore unnecessary to the human diet. Food with higher amounts of dietary fiber take longer to cook and have a much shorter shelf life. In recent times, dietary fiber has been identified as an important component of the human diet and a daily uptake at least 30g of dietary fiber is recommended, see Dietary Reference Intake.
Two types of dietary fiber are roughly distinguished: water soluble and water insoluble fiber. Both types have different effects on digestion, e.g. not all dietary fiber lead to the same degree to flatulence.
Dietary fibers can act by changing the nature of the contents of the gastrointestinal tract and by changing how other nutrients and chemicals are absorbed.[1] Some types of soluble fiber absorb water to become a gelatinous, viscous substance which is fermented by bacteria in the digestive tract. Some types of insoluble fiber have bulking action and are not fermented.[2] Lignin, a major dietary insoluble fiber source, may alter the rate and metabolism of soluble fibers.[3] Other types of insoluble fiber, notably resistant starch, are fully fermented.[4]
Chemically, dietary fiber consists of non-starch polysaccharides such as arabinoxylans, cellulose, and many other plant components such as resistant starch, resistant dextrins, inulin, lignin, waxes, chitins, pectins, beta-glucans, and oligosaccharides.[3] A novel position has been adopted by the US Department of Agriculture to include functional fibers as isolated fiber sources that may be included in the diet.[3] The term "fiber" is something of a misnomer, since many types of so-called dietary fiber are not actually fibrous.
Food sources of dietary fiber are often divided according to whether they provide (predominantly) soluble or insoluble fiber. Plant foods contain both types of fiber in varying degrees, according to the plant's characteristics.
Advantages of consuming fiber are the production of healthful compounds during the fermentation of soluble fiber, and insoluble fiber's ability (via its passive hygroscopic properties) to increase bulk, soften stool, and shorten transit time through the intestinal tract.
A disadvantage of a diet high in fiber is the potential for significant intestinal gas production and bloating. Constipation can occur if insufficient fluid is consumed with a high-fiber diet.
Definition
[edit]Originally, fiber was defined to be the components of plants that resist human digestive enzymes, enzymatic break-down usually being prerequisite prior to the absorption into the blood stream; this definition that includes lignin and polysaccharides. The definition was later changed to also include resistant starch, along with inulin and other oligosaccharides.[2]
The amount of dietary fiber declared on the nutrition facts label is subject to legal provisions. Official definition of dietary fiber differs a little among different institutions:
| Organization (reference) | Definition |
|---|---|
| Institute of Medicine[5] | Dietary fiber consists of nondigestible carbohydrates and lignin that are intrinsic and intact in plants. Functional fiber consists of isolated, nondigestible carbohydrates that have beneficial physiologic effects in humans. Total fiber is the sum of dietary fiber and functional fiber. |
| American Association of Cereal Chemists[6] | Dietary fiber is the edible parts of plants or analogous carbohydrates that are resistant to digestion and absorption in the human small intestine, with complete or partial fermentation in the large intestine. Dietary fiber includes polysaccharides, oligosaccharides, lignin, and associated plant substances. Dietary fibers promote beneficial physiologic effects including laxation, and/or blood cholesterol attenuation, and/or blood glucose attenuation. |
| Codex Alimentarius Commission[7] | Dietary fiber means carbohydrate polymers with ≥10 monomeric units, which are not hydrolyzed by the endogenous enzymes in the small intestine of humans. |
Nutrition physiology
[edit]Types and sources of dietary fiber
[edit]Types
[edit]- soluble fiber is readily fermented in the large intestine (colon) into gases and physiologically active byproducts, and can be prebiotic and viscous. Soluble fibers tend to slow the movement of food through the system.
- insoluble fiber, which does not dissolve in water. It can be metabolically inert and provide bulking, or it can be prebiotic and metabolically ferment in the large intestine. Bulking fibers absorb water as they move through the digestive system, easing defecation.[3] Fermentable insoluble fibers mildly promote stool regularity, although not to the extent that bulking fibers do, but they can be readily fermented in the colon into gases and physiologically active byproducts. Insoluble fibers tend to accelerate the movement of food through the system.
Table
[edit]| Nutrient | Food additive | appearance / preparation |
| water insoluble dietary fibers | ||
| β-glucans (a few of which are water soluble) | ||
| Cellulose | E 460 | cereals, fruit, vegetables (in all plants in general) |
| Chitin | — | in fungi, exoskeleton of insects and crustaceans |
| Hemicellulose | cereals, bran, timber, legume | |
| Hexosane | — | wheat, barley |
| Pentosane | — | rye, oat |
| Lignin | — | stones of fruits, vegetables (filaments of the garden bean), cereals |
| Xanthan | E 415 | production with Xanthomonas-bacteria from sugar substrates |
| water soluble dietary fibers | ||
| Fructans | replace or complement in some plant taxa the starch as storage carbohydrate | |
| Inulin | — | storage carbohydrate in diverse plants, e.g. topinambour, chicory, etc. |
| Polyuronide | ||
| Pectin | E 440 | in the fruit skin (mainly apples, quinces), vegetables |
| Alginic acids (Alginates) | E 400–E 407 | in Algae |
| Natriumalginat | E 401 | |
| Kaliumalginat | E 402 | |
| Ammoniumalginat | E 403 | |
| Calciumalginat | E 404 | |
| Propylenglycolalginat (PGA) | E 405 | |
| agar | E 406 | |
| carrageen | E 407 | red algae |
| Raffinose | — | storage carbohydrate in legumes |
| Polydextrose | E 1200 | synthetic polymer, ca. 1kcal/g |
| Lactulose | — | synthetic disaccharide |
Fiber contents in food
[edit]Dietary fibers are found in fruits, vegetables and whole grains. The exact amount of fiber contained in the food can be seen in the following table of expected fiber in USDA food groups/subgroups[8]
| Food group | Serving Mean | fiber g/serving |
| Fruit | 0.5 cup | 1.1 |
| Dark-green vegetables | 0.5 cup | 6.4 |
| Orange vegetables | 0.5 cup | 2.1 |
| Cooked dry beans (legumes) | 0.5 cup | 8.0 |
| Starchy vegetables | 0.5 cup | 1.7 |
| Other vegetables | 0.5 cup | 1.1 |
| Whole grains | 28 g (1 oz) | 2.4 |
| Meat | 28 g (1 oz) | 0.1 |
Dietary fiber is found in plants. While all plants contain some fiber, plants with high fiber concentrations are generally the most practical source.
Fiber-rich plants can be eaten directly. Or, alternatively, they can be used to make supplements and fiber-rich processed foods.
The Academy of Nutrition and Dietetics (AND), formerly the American Dietetic Association, recommends consuming a variety of fiber-rich foods.
Plant sources of fiber
[edit]
Some plants contain significant amounts of soluble and insoluble fiber. For example plums and prunes have a thick skin covering a juicy pulp. The skin is a source of insoluble fiber, whereas soluble fiber is in the pulp. Grapes also contain a fair amount of fiber.[9]
The root of the konjac plant, or glucomannan, produces results similar to fiber and may also be used to relieve constipation. Glucomannan is sold in various forms, and while safe in some forms, it can be unsafe in others, possibly leading to throat or intestinal blockage.[10]
Soluble fiber is found in varying quantities in all plant foods, including:
- legumes (peas, soybeans, lupins and other beans)
- oats, rye, chia, and barley
- some fruits (including figs, avocados, plums, prunes, berries, ripe bananas, and the skin of apples, quinces and pears)
- certain vegetables such as broccoli, carrots, and Jerusalem artichokes
- root tubers and root vegetables such as sweet potatoes and onions (skins of these are sources of insoluble fiber also)
- psyllium seed husks (a mucilage soluble fiber) and flax seeds
- nuts, with almonds being the highest in dietary fiber
Sources of insoluble fiber include:
- whole grain foods
- wheat and corn bran
- legumes such as beans and peas
- nuts and seeds
- potato skins
- lignans
- vegetables such as green beans, cauliflower, zucchini (courgette), celery, and nopal
- some fruits including avocado, and unripe bananas
- the skins of some fruits, including kiwifruit, grapes and tomatoes[11]
Fiber supplements
[edit]These are a few example forms of fiber that have been sold as supplements or food additives. These may be marketed to consumers for nutritional purposes, treatment of various gastrointestinal disorders, and for such possible health benefits as lowering cholesterol levels, reducing risk of colon cancer, and losing weight.
Soluble fiber supplements may be beneficial for alleviating symptoms of irritable bowel syndrome, such as diarrhea or constipation and abdominal discomfort.[12] Prebiotic soluble fiber products, like those containing inulin or oligosaccharides, may contribute to relief from inflammatory bowel disease,[13] as in Crohn's disease,[14] ulcerative colitis,[15][16] and Clostridium difficile,[17] due in part to the short-chain fatty acids produced with subsequent anti-inflammatory actions upon the bowel.[18][19] Fiber supplements may be effective in an overall dietary plan for managing irritable bowel syndrome by modification of food choices.[20]
One insoluble fiber, resistant starch from high amylose corn, has been used as a supplement and may contribute to improving insulin sensitivity and glycemic management[21][22][23] as well as promoting regularity[24] and possibly relief of diarrhea.[25][26][27] One preliminary finding indicates that resistant corn starch may reduce symptoms of ulcerative colitis.[28]
Inulins
[edit]Chemically defined as oligosaccharides occurring naturally in most plants, inulins have nutritional value as carbohydrates, or more specifically as fructans, a polymer of the natural plant sugar, fructose. Inulin is typically extracted by manufacturers from enriched plant sources such as chicory roots or Jerusalem artichokes for use in prepared foods.[29] Subtly sweet, it can be used to replace sugar, fat, and flour, is often used to improve the flow and mixing qualities of powdered nutritional supplements, and has significant potential health value as a prebiotic fermentable fiber.[30]
Inulin is advantageous because it contains 25–30% the food energy of sugar or other carbohydrates and 10–15% the food energy of fat. As a prebiotic fermentable fiber, its metabolism by gut flora yields short-chain fatty acids (see below) which increase absorption of calcium,[31] magnesium,[32] and iron,[33] resulting from upregulation of mineral-transporting genes and their membrane transport proteins within the colon wall. Among other potential beneficial effects noted above, inulin promotes an increase in the mass and health of intestinal Lactobacillus and Bifidobacterium populations.
Vegetable gums
[edit]Vegetable gum fiber supplements are relatively new to the market. Often sold as a powder, vegetable gum fibers dissolve easily with no aftertaste. In preliminary clinical trials, they have proven effective for the treatment of irritable bowel syndrome.[34] Examples of vegetable gum fibers are guar gum and acacia Senegal gum.
Digestion of dietary fibers: mechanisms of action
[edit]Dietary fibers have three primary mechanisms: bulking, viscosity and fermentation.[35] Dietary fibers can change the nature of the contents of the gastrointestinal tract, and to change how other nutrients and chemicals are absorbed through bulking and viscosity.[3][1] Some types of soluble fibers bind to bile acids in the small intestine, making them less likely to re-enter the body; this in turn lowers cholesterol levels in the blood from the actions of cytochrome P450-mediated oxidation of cholesterol.[2] Viscous soluble fibers may also attenuate the absorption of sugar, reduce sugar response after eating, normalize blood lipid levels and, once fermented in the colon, produce short-chain fatty acids as byproducts with wide-ranging physiological activities (discussion below). Insoluble fiber is associated with reduced diabetes risk, but the mechanism by which this occurs is unknown.[36] One type of insoluble dietary fiber, resistant starch has been shown to directly increase insulin sensitivity in healthy people,[37][38] in type 2 diabetics,[39] and in individuals with insulin resistance, possibly contributing to reduced risk of type 2 diabetes.[40][41][42]
Not yet formally proposed as an essential macro-nutrient, dietary fiber is nevertheless regarded as important for the diet, with regulatory authorities in many developed countries recommending increases in fiber intake.[3][1][43][44]
Physicochemical properties
[edit]Dietary fiber has distinct physicochemical properties. Most semi-solid foods, fiber and fat are a combination of gel matrices which are hydrated or collapsed with microstructural elements, globules, solutions or encapsulating walls. Fresh fruit and vegetables are cellular materials.[45][46][47]
- The cells of cooked potatoes and legumes are gels filled with gelatinized starch granules. The cellular structures of fruits and vegetables are foams with a closed cell geometry filled with a gel, surrounded by cell walls which are composites with an amorphous matrix strengthened by complex carbohydrate fibers.
- Particle size and interfacial interactions with adjacent matrices affect the mechanical properties of food composites.
- Food polymers may be soluble in and/or plasticized by water. Water is the most important plasticizer, particularly in biological systems thereby changing mechanical properties.
- The variables include chemical structure, polymer concentration, molecular weight, degree of chain branching, the extent of ionization (for electrolytes), solution pH, ionic strength and temperature.
- Cross-linking of different polymers, protein and polysaccharides, either through chemical covalent bonds or cross-links through molecular entanglement or hydrogen or ionic bond cross-linking.
- Cooking and chewing food alters these physicochemical properties and hence absorption and movement through the stomach and along the intestine[48]
Dietary fiber and the upper gastrointestinal tract
[edit]A slowly eaten meal will enter the absorptive phase of the gastrointestinal tract more slowly than a rapidly eaten meal of similar composition. Many of the differences between low and high glycemic foods would disappear if a meal was eaten slowly.[49][50]
The chemical and physico-chemical nature (lipid, protein, carbohydrate) of the meal will also influence the gastric emptying of the food multiphase system. Fatty foods and hypertonic solutions empty slowly. The movement of food, i.e., chyme, along the gastrointestinal tract is typical of flow in a disperse system. As chyme moves along the gastrointestinal tract, polymer flow and diffusion becomes important.[51]
Following a meal, the stomach and upper gastrointestinal contents consist of
- food compounds
- complex lipids/micellar/aqueous/hydrocolloid and hydrophobic phases
- hydrophilic phases
- solid, liquid, colloidal and gas bubble phases.[52]
Micelles are colloid-sized clusters of molecules which form in conditions as those above, similar to the critical micelle concentration of detergents.[53] In the upper gastrointestinal tract, these detergents consist of bile acids and di- and monoacyl glycerols which solubilize triacylglycerols and cholesterol.[53]
Two mechanisms bring nutrients into contact with the epithelium:
- intestinal contractions create turbulence; and
- convection currents direct contents from the lumen to the epithelial surface.[51]
The multiple physical phases in the intestinal tract slow the rate of absorption compared to that of the suspension solvent alone.
- Nutrients diffuse through the thin, relatively unstirred layer of fluid adjacent to the epithelium.
- Immobilizing of nutrients and other chemicals within complex polysaccharide molecules affects their release and subsequent absorption from the small intestine, an effect influential on the glycemic index.[51]
- Molecules begin to interact as their concentration increases. During absorption, water must be absorbed at a rate commensurate with the absorption of solutes. The transport of actively and passively absorbed nutrients across epithelium is affected by the unstirred water layer covering the microvillus membrane.[51]
- The presence of mucus or fiber, e.g., pectin or guar, in the unstirred layer may alter the viscosity and solute diffusion coefficient.[52]
Adding viscous polysaccharides to carbohydrate meals can reduce post-prandial blood glucose concentrations. Wheat and maize but not oats modify glucose absorption, the rate being dependent upon the particle size. The reduction in absorption rate with guar gum may be due to the increased resistance by viscous solutions to the convective flows created by intestinal contractions. Dietary fiber interacts with pancreatic and enteric enzymes and their substrates. Human pancreatic enzyme activity is reduced when incubated with most fiber sources. Fiber may affect amylase activity and hence the rate of hydrolysis of starch. The more viscous polysaccharides extend the mouth-to-cecum transit time; guar, tragacanth and pectin being slower than wheat bran.[54]
Fiber in the colon
[edit]Even Termites have to rely on microorganism to digest cellulose.
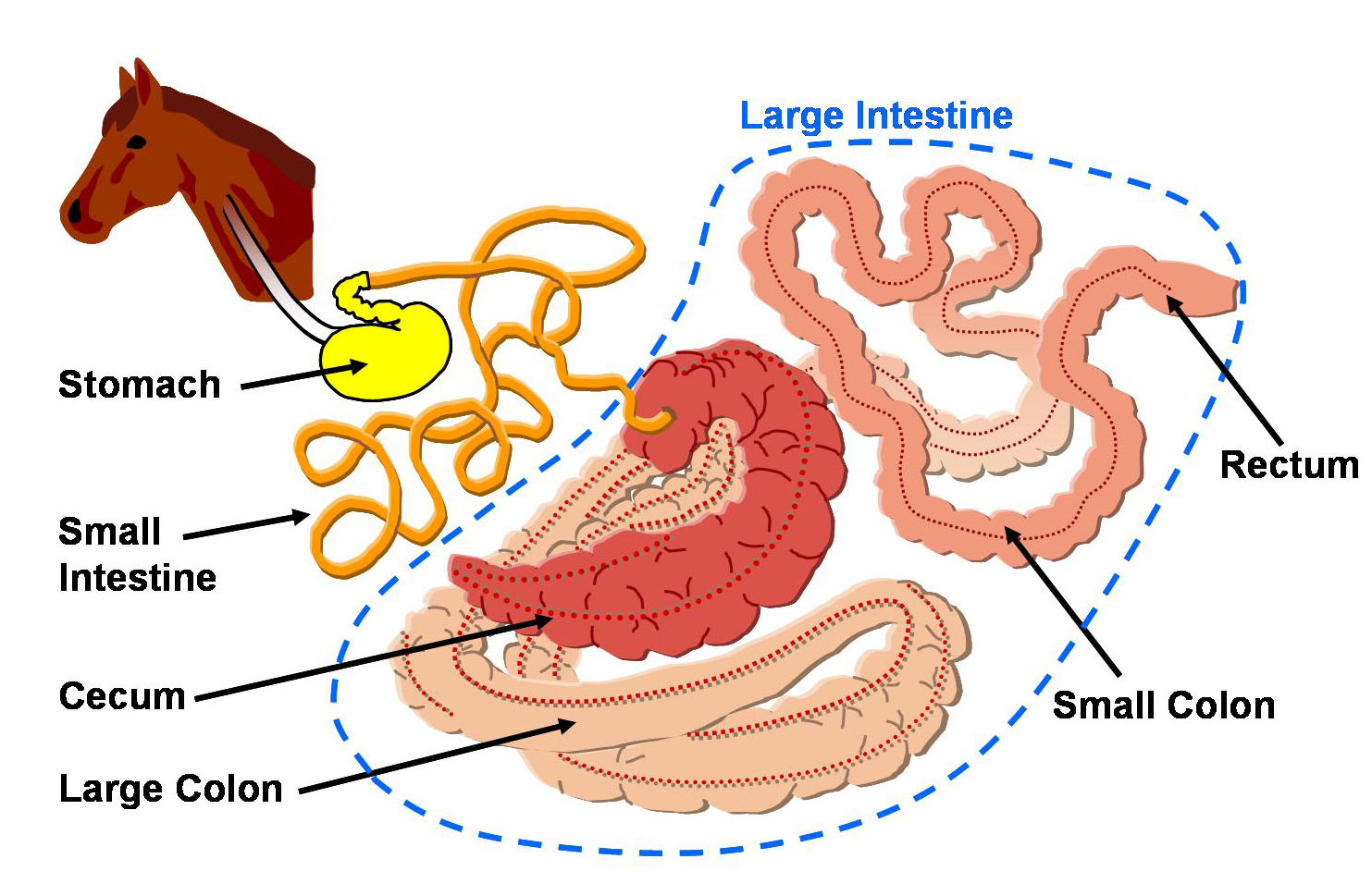
In non-ruminantia, the colon (large intestine) play's a dominant role in the digestion of dietary fiber. Anatomically, the colon is usually divided into 5 sections with a differentiating role in the digestion of dietary fiber:
- the Cecum
- in foregut fermenter (e.g. ruminatia), a trait that evolved after the spread of the C4-grasses and probably also after the horse-like grass-eaters, still feature an enlarged cecum. However, since the majority of the digestion takes place in the rumen, more gas is passed through burping than through farting.
- in hindgut fermenter such as e.g. horses, which are non-ruminatian herbivores, who's diet consist to a large portion of grasses containing high amounts of cellulose, the cecum is proportionally noticeably enlarged.[55] It serves as the main fermenter, where the break-down of the cellulose and other dietary fibers is performed by bacteria. Horses are known to excrete two kinds of excrement, one kind called cecotrope being reused as protein rich food consisted of bacteria and easily absorbable carbohydrates.[56]
- in humans and other omnivores, the cecum has the same function, but due to the much lower amounts of grass in the diet it is not as enlarged as in horses.
The right side of the colon is involved in nutrient salvage so that dietary fiber, resistant starch, fat and protein are utilized by bacteria and the end-products absorbed for use by the body
- the left side (transverse, descending, sigmoid colon, affecting continence.
The presence of bacteria in the colon produces an ‘organ’ of intense, mainly reductive, metabolic activity, whereas the liver is oxidative. The substrates utilized by the cecal have either passed along the entire intestine or are biliary excretion products. The effects of dietary fiber in the colon are on
- bacterial fermentation of some dietary fibers
- thereby an increase in bacterial mass
- an increase in bacterial enzyme activity
- changes in the water-holding capacity of the fiber residue after fermentation
Enlargement of the cecum is a common finding when some dietary fibers are fed and this is now believed to be normal physiological adjustment. Such an increase may be due to a number of factors, prolonged cecal residence of the fiber, increased bacterial mass, or increased bacterial end-products. Some non-absorbed carbohydrates, e.g. pectin, gum arabic, oligosaccharides and resistant starch, are fermented to short-chain fatty acids (chiefly acetic, propionic and n-butyric), and carbon dioxide, hydrogen and methane. The cecal fermentation of 40–50 g of complex polysaccharides will yield 400–500 mmol total short-chain fatty acids, 240–300 mmol acetate, and 80–100 mmol of both propionate and butyrate.[citation needed] Almost all of these short-chain fatty acids will be absorbed from the colon. This means that fecal short-chain fatty acid estimations do not reflect cecal and colonic fermentation, only the efficiency of absorption, the ability of the fiber residue to sequestrate short-chain fatty acids, and the continued fermentation of fiber around the colon, which presumably will continue until the substrate is exhausted. The production of short-chain fatty acids has several possible actions on the gut mucosa. All of the short-chain fatty acids are readily absorbed by the colonic mucosa, but only acetic acid reaches the systemic circulation in appreciable amounts. Butyric acid appears to be used as a fuel by the colonic mucosa as the preferred energy source for colonic cells.
Dietary fiber and cholesterol metabolism
[edit]Dietary fiber may act on each phase of ingestion, digestion, absorption and excretion to affect cholesterol metabolism,[57] such as the following:
- Caloric energy of foods through a bulking effect
- Slowing of gastric emptying time
- A glycemic index type of action on absorption
- A slowing of bile acid absorption in the ileum so bile acids escape through to the cecum
- Altered or increased bile acid metabolism in the cecum
- Indirectly by absorbed short-chain fatty acids, especially propionic acid, resulting from fiber fermentation affecting the cholesterol metabolism in the liver.
- Binding of bile acids to fiber or bacteria in the cecum with increased fecal loss from the entero-hepatic circulation.
An important action of some fibers is to reduce the reabsorption of bile acids in the ileum and hence the amount and type of bile acid and fats reaching the colon. A reduction in the reabsorption of bile acid from the ileum has several direct effects.
- Bile acids may be trapped within the lumen of the ileum either because of a high luminal viscosity or because of binding to a dietary fiber.[58]
- Lignin in fiber adsorbs bile acids, but the unconjugated form of the bile acids are adsorbed more than the conjugated form. In the ileum where bile acids are primarily absorbed the bile acids are predominantly conjugated.
- The enterohepatic circulation of bile acids may be altered and there is an increased flow of bile acids to the cecum, where they are deconjugated and 7alpha-dehydroxylated.
- These water-soluble form, bile acids e.g., deoxycholic and lithocholic are adsorbed to dietary fiber and an increased fecal loss of sterols, dependent in part on the amount and type of fiber.
- A further factor is an increase in the bacterial mass and activity of the ileum as some fibers e.g., pectin are digested by bacteria. The bacterial mass increases and cecal bacterial activity increases.
- The enteric loss of bile acids results in increased synthesis of bile acids from cholesterol which in turn reduces body cholesterol.
The fibers that are most effective in influencing sterol metabolism (e.g. pectin) are fermented in the colon. It is therefore unlikely that the reduction in body cholesterol is due to adsorption to this fermented fiber in the colon.
- There might be alterations in the end-products of bile acid bacterial metabolism or the release of short chain fatty acids which are absorbed from the colon, return to the liver in the portal vein and modulate either the synthesis of cholesterol or its catabolism to bile acids.
- The prime mechanism whereby fiber influences cholesterol metabolism is through bacteria binding bile acids in the colon after the initial deconjugation and dehydroxylation.[59]
- Fermentable fibers e.g., pectin will by virtue of their providing a medium for bacterial growth increase the bacterial mass in the colon. The sequestrated bile acids are then excreted in feces.
- Other fibers, e.g., gum arabic, act as stabilizers and cause a significant decrease in serum cholesterol without increasing fecal bile acid excretion.
Dietary fiber and fecal weight
[edit]Feces consist of plasticine-like material, made up of water, bacteria, lipids, sterols, mucus and fiber.
- Feces are 75% water; bacteria make a large contribution to the dry weight, the residue being unfermented fiber and excreted compounds.
- Fecal output may vary over a range of between 20 and 280 g over 24 hours. The amount of feces egested a day varies for any one individual over a period of time.
- Of dietary constituents, only dietary fiber increases fecal weight.
Water is distributed in the colon in three ways:
- Free water which can be absorbed from the colon.
- Water that is incorporated into bacterial mass.
- Water that is bound by fiber.
Fecal weight is dictated by:
- the holding of water by the residual dietary fiber after fermentation.
- the bacterial mass.
- There may also be an added osmotic effect of products of bacterial fermentation on fecal mass.
Wheat bran is minimally fermented and binds water and when added to the diet increases fecal weight in a predictable linear manner and decreases intestinal transit time. The particle size of the fiber is all-important, coarse wheat bran being more effective than fine wheat bran. The greater the water-holding capacity of the bran, the greater the effect on fecal weight. For most healthy individuals, an increase in wet fecal weight, depending on the particle size of the bran, is generally of the order of 3–5 g/g fiber. The fermentation of some fibers results in an increase in the bacterial content and possibly fecal weight. Other fibers, e.g. pectin, are fermented and have no effect on stool weight.
All sorts of claims and bla
[edit]Effects of fiber intake
[edit]Research has shown that fiber may benefit health in several different ways. Lignin and probably related materials that are resistant to enzymatic degradation, diminish the nutritional value of foods.[60]
Table legend
[edit]Color coding of table entries:
- Both Applies to both soluble and insoluble fiber
- Soluble Applies to soluble fiber only
- Insoluble Applies to insoluble fiber only
| Effects[61][62] |
|---|
| Increases food volume without increasing caloric content to the same extent as digestible carbohydrates, providing satiety which may reduce appetite. |
| Attracts water and forms a viscous gel during digestion, slowing the emptying of the stomach and intestinal transit, shielding carbohydrates from enzymes, and delaying absorption of glucose,[63] which lowers variance in blood sugar levels |
| Lowers total and LDL cholesterol, which may reduce the risk of cardiovascular disease |
| Regulates blood sugar, which may reduce glucose and insulin levels in diabetic patients and may lower risk of diabetes[64] |
| Speeds the passage of foods through the digestive system, which facilitates regular defecation |
| Adds bulk to the stool, which alleviates constipation |
| Balances intestinal pH[65] and stimulates intestinal fermentation production of short-chain fatty acids, which may reduce risk of colorectal cancer[66] |
Fiber does not bind to minerals and vitamins and therefore does not restrict their absorption, but rather evidence exists that fermentable fiber sources improve absorption of minerals, especially calcium.[67][68][69] Some plant foods can reduce the absorption of minerals and vitamins like calcium, zinc, vitamin C, and magnesium, but this is caused by the presence of phytate (which is also thought to have important health benefits), not by fiber.[70]
An experiment designed with a large sample and conducted by NIH-AARP Diet and Health Study studied the correlation between fiber intake and colorectal cancer. The analytic cohort consisted of 291 988 men and 197 623 women aged 50–71 y. Diet was assessed with a self-administered food-frequency questionnaire at baseline in 1995-1996; 2974 incident colorectal cancer cases were identified during 5 y of follow-up. The result was that total fiber intake was not associated with colorectal cancer. But on the other hand, the analyses of fiber from different food sources showed that fiber from grains was associated with a lower risk of colorectal cancer.[71]
Although many researchers believe that dietary fiber intake reduces risk of colon cancer, one study conducted by researchers at the Harvard School of Medicine of over 88,000 women did not show a statistically significant relationship between higher fiber consumption and lower rates of colorectal cancer or adenomas.[72] Similarly, a 2010 study of 58,279 men found no relationship between dietary fiber and colorectal cancer.[73]
Dietary fiber and obesity
[edit]Dietary fiber has many functions in diet, one of which may be to aid in energy intake control and reduced risk for development of obesity. The role of dietary fiber in energy intake regulation and obesity development is related to its unique physical and chemical properties that aid in early signals of satiation and enhanced or prolonged signals of satiety. Early signals of satiation may be induced through cephalic- and gastric-phase responses related to the bulking effects of dietary fiber on energy density and palatability, whereas the viscosity-producing effects of certain fibers may enhance satiety through intestinal-phase events related to modified gastrointestinal function and subsequent delay in fat absorption. In general, fiber-rich diets, whether achieved through fiber supplementation or incorporation of high fiber foods into meals, have a reduced energy density compared with high fat diets. This is related to fiber’s ability to add bulk and weight to the diet. There are also indications that women may be more sensitive to dietary manipulation with fiber than men. The relationship of body weight status and fiber effect on energy intake suggests that obese individuals may be more likely to reduce food intake with dietary fiber inclusion.[74]
Guidelines on fiber intake
[edit]Current recommendations from the United States National Academy of Sciences, Institute of Medicine, suggest that adults should consume 20–35 grams of dietary fiber per day, but the average American's daily intake of dietary fiber is only 12–18 grams.[70][75]
The AND (Academy of Nutrition and Dietetics, previously ADA) recommends a minimum of 20–35 g/day for a healthy adult depending on calorie intake (e.g., a 2000 Cal/8400 kJ diet should include 25 g of fiber per day). The AND's recommendation for children is that intake should equal age in years plus 5 g/day (e.g., a 4 year old should consume 9 g/day). No guidelines have yet been established for the elderly or very ill. Patients with current constipation, vomiting, and abdominal pain should see a physician. Certain bulking agents are not commonly recommended with the prescription of opioids because the slow transit time mixed with larger stools may lead to severe constipation, pain, or obstruction.
The British Nutrition Foundation has recommended a minimum fiber intake of 18 g/day for healthy adults.[76]
United States
[edit]On average, North Americans consume less than 50% of the dietary fiber levels recommended for good health. In the preferred food choices of today's youth, this value may be as low as 20%, a factor considered by experts as contributing to the obesity levels seen in many developed countries.[77][78]
The actual fiber intake gaps of different age groups of Americans are shown in the graph from USDA:

Recognizing the growing scientific evidence for physiological benefits of increased fiber intake, regulatory agencies such as the Food and Drug Administration (FDA) of the United States have given approvals to food products making health claims for fiber.
In clinical trials to date, these fiber sources were shown to significantly reduce blood cholesterol levels, an important factor for general cardiovascular health,[80] and to lower risk of onset for some types of cancer.[81]
Soluble (fermentable) fiber sources gaining FDA approval are:
- Psyllium seed husk (7 grams per day)
- Beta-glucan from oat bran, whole oats, oatrim, or rolled oats (3 grams per day)
- Beta-glucan from whole grain or dry-milled barley (3 grams per day)
Other examples of fermentable fiber sources (from plant foods or biotechnology) used in functional foods and supplements include inulin, resistant dextrins, fructans, xanthan gum, cellulose, guar gum, fructooligosaccharides (FOS), and oligo- or polysaccharides.
Consistent intake of fermentable fiber through foods like berries and other fresh fruit, vegetables, whole grains, seeds, and nuts is now known to reduce risk of some of the world’s most prevalent diseases[82][83][84][85]—obesity, diabetes, high blood cholesterol, cardiovascular disease, and numerous gastrointestinal disorders. In this last category are constipation, inflammatory bowel disease, ulcerative colitis, hemorrhoids, Crohn's disease, diverticulitis, and colon cancer—all disorders of the intestinal tract where fermentable fiber can provide healthful benefits.[82]
Insufficient fiber in the diet can complicate defecation.[86] Low-fiber feces are dehydrated and hardened, making them difficult to evacuate—defining constipation[86] and possibly leading to development of hemorrhoids[86] or anal fissures.
In 2014, the International Scientific Association for Probiotics and Prebiotics submitted a petition to the Food and Drug Administration expanding the physiological effects of fiber consumption to the bulleted list below.[87]
Great Britain
[edit]In June 2007, the British Nutrition Foundation issued a statement to define dietary fiber more concisely and list the potential health benefits established to date.[88][89] Statement: ‘Dietary fibre’ has been used as a collective term for a complex mixture of substances with different chemical and physical properties which exert different types of physiological effects.
The use of certain analytical methods to quantify dietary fiber by nature of its indigestibility results in many other indigestible components being isolated along with the carbohydrate components of dietary fiber. These components include resistant starches and oligosaccharides along with other substances that exist within the plant cell structure and contribute to the material that passes through the digestive tract. Such components are likely to have physiological effects.
Yet, some differentiation has to be made between these indigestible plant components and other partially digested material, such as protein, that appears in the large bowel. Thus, it is better to classify fiber as a group of compounds with different physiological characteristics, rather than to be constrained by defining it chemically (end quote).
Diets naturally high in fiber can be considered to bring about several main physiological consequences:
- increases fecal bulk and helps prevent constipation by decreasing fecal transit time in the large intestine
- reduces blood pressure
- improves gastrointestinal health
- improves glucose tolerance and the insulin response following a meal
- increases colonic fermentation and short-chain fatty acid production
- positively modulates colonic microflora
- reduces hyperlipidemia, hypertension, and other coronary heart disease risk factors
- reduces the risk of developing some cancers, particularly colon cancer
- increases satiety and hence some degree of weight management
Therefore, it is not appropriate to state that fiber has a single all-encompassing physiological property as these effects are dependent on the type of fiber in the diet. The beneficial effects of high fiber diets are the summation of the effects of the different types of fiber present in the diet and also other components of such diets.
Defining fiber physiologically allows recognition of indigestible carbohydrates with structures and physiological properties similar to those of naturally occurring dietary fibers.[89]
FDA-approved health claims
[edit]The FDA allows producers of foods containing 1.7g per serving of psyllium husk soluble fiber or 0.75g of oat or barley soluble fiber as beta-glucans to claim that reduced risk of heart disease can result from their regular consumption.[90]
The FDA statement template for making this claim is: Soluble fiber from foods such as [name of soluble fiber source, and, if desired, name of food product], as part of a diet low in saturated fat and cholesterol, may reduce the risk of heart disease. A serving of [name of food product] supplies __ grams of the [necessary daily dietary intake for the benefit] soluble fiber from [name of soluble fiber source] necessary per day to have this effect.[90]
Eligible sources of soluble fiber providing beta-glucan include:
- Oat bran
- Rolled oats
- Whole oat flour
- Oatrim
- Whole grain barley and dry milled barley
- Soluble fiber from psyllium husk with purity of no less than 95%
The allowed label may state that diets low in saturated fat and cholesterol and that include soluble fiber from certain of the above foods "may" or "might" reduce the risk of heart disease.
As discussed in FDA regulation 21 CFR 101.81, the daily dietary intake levels of soluble fiber from sources listed above associated with reduced risk of coronary heart disease are:
- 3g or more per day of beta-glucan soluble fiber from either whole oats or barley, or a combination of whole oats and barley
- 7g or more per day of soluble fiber from psyllium seed husk.[91]
Soluble fiber from consuming grains is included in other allowed health claims for lowering risk of some types of cancer and heart disease by consuming fruit and vegetables (21 CFR 101.76, 101.77, and 101.78).[90]
Potential longevity
[edit]A study of 388,000 adults ages 50 to 71 for nine years found that the highest consumers of fiber were 22% less likely to die over this period.[92] In addition to lower risk of death from heart disease, adequate consumption of fiber-containing foods, especially grains, was also associated with reduced incidence of infectious and respiratory illnesses, and, particularly among males, reduced risk of cancer-related death.
Fiber and calories
[edit]Fiber contributes less energy—usually measured in kilojoules (kJ) or kilocalories (kcal), also known as dietary Calories (Cal)—than sugars and starches because it cannot be fully absorbed by the body. Sugars and starches provide 17 kJ/g (4.1 kcal/g),[93] and the human body has specific enzymes to break them down into glucose, fructose, and galactose, which can then be absorbed by the body. The human body lacks enzymes to break down fiber. Insoluble fiber does not change inside the body, so the body cannot absorb it and it provides no energy. Soluble fiber is partially fermented, with the degree of fermentability varying with the type of fiber, and contributes some energy when broken down and absorbed by the body. Dietitians have not reached a consensus on how much energy is actually absorbed, but some approximate 8 kJ/g (1.9 kcal/g). Regardless of the type of fiber, the body absorbs less than 17 kJ/g (4.1 kcal/g), which can create inconsistencies for actual product nutrition labels. In some countries fiber is not listed on nutrition labels and is considered to provide no energy. In other countries all fiber must be listed and is simplistically considered to provide 17 kJ/g (4.1 kcal/g) (because chemically fiber is a type of carbohydrate and other carbohydrates provide that amount of energy). In the US, soluble fiber must be counted as 4 kcal/g (17 kJ/g), but insoluble fiber may be (and usually is) treated as not providing energy and not mentioned on the label.
Soluble fiber fermentation
[edit]The American Association of Cereal Chemists has defined soluble fiber this way: "the edible parts of plants or similar carbohydrates resistant to digestion and absorption in the human small intestine with complete or partial fermentation in the large intestine."[94] In this definition:
- edible parts of plants
- indicates that some parts of a plant we eat—skin, pulp, seeds, stems, leaves, roots—contain fiber. Both insoluble and soluble sources are in those plant components.
- carbohydrates
- complex carbohydrates, such as long-chained sugars also called starch, oligosaccharides, or polysaccharides, are sources of soluble fermentable fiber.
- resistant to digestion and absorption in the human small intestine
- foods providing nutrients are digested by gastric acid and digestive enzymes in the stomach and small intestine where the nutrients are released then absorbed through the intestinal wall for transport via the blood throughout the body. A food resistant to this process is undigested, as insoluble and soluble fibers are. They pass to the large intestine only affected by their absorption of water (insoluble fiber) or dissolution in water (soluble fiber).
- complete or partial fermentation in the large intestine
- the large intestine comprises a segment called the colon within which additional nutrient absorption occurs through the process of fermentation. Fermentation occurs by the action of colonic bacteria on the food mass, producing gases and short-chain fatty acids. It is these short-chain fatty acids—butyric, acetic (ethanoic), propionic, and valeric acids—that scientific evidence is revealing to have significant health properties.[95]
As an example of fermentation, shorter-chain carbohydrates (a type of fiber found in legumes) cannot be digested, but are changed via fermentation in the colon into short-chain fatty acids and gases (which are typically expelled as flatulence).
According to a 2002 journal article,[82] fibers compounds with partial or low fermentability include:
- cellulose, a polysaccharide
- hemicellulose, a polysaccharide
- lignans, a group of phytoestrogens
- plant waxes
- resistant starches
fiber compounds with high fermentability include:
- beta-glucans, a group of polysaccharides
- pectins, a group of heteropolysaccharides
- natural gums, a group of polysaccharides
- inulins, a group of polysaccharides
- oligosaccharides, a group of short-chained or simple sugars
- resistant dextrins[96]
Short-chain fatty acids
[edit]When soluble fiber is fermented, short-chain fatty acids (SCFA) are produced. SCFAs are involved in numerous physiological processes promoting health, including:[95]
- stabilize blood glucose levels by acting on pancreatic insulin release and liver control of glycogen breakdown
- stimulate gene expression of glucose transporters in the intestinal mucosa, regulating glucose absorption[97]
- provide nourishment of colonocytes, particularly by the SCFA butyrate
- suppress cholesterol synthesis by the liver and reduce blood levels of LDL cholesterol and triglycerides responsible for atherosclerosis
- lower colonic pH (i.e., raises the acidity level in the colon) which protects the lining from formation of colonic polyps and increases absorption of dietary minerals
- stimulate production of T helper cells, antibodies, leukocytes, cytokines, and lymph mechanisms having crucial roles in immune protection
- improve barrier properties of the colonic mucosal layer, inhibiting inflammatory and adhesion irritants, contributing to immune functions
SCFAs that are absorbed by the colonic mucosa pass through the colonic wall into the portal circulation (supplying the liver), and the liver transports them into the general circulatory system.
Overall, SCFAs affect major regulatory systems, such as blood glucose and lipid levels, the colonic environment, and intestinal immune functions.[98][99]
The major SCFAs in humans are butyrate, propionate, and acetate, where butyrate is the major energy source for colonocytes, propionate is destined for uptake by the liver, and acetate enters the peripheral circulation to be metabolized by peripheral tissues.
See also
[edit]- Nutrient
- Essential nutrient
- List of macronutrients
- List of micronutrients
- List of phytochemicals in food
- Underweight
- High residue diet
- Low residue diet
- Methylcellulose
- Prebiotic—indigestible matter which encourages growth of gut flora
- Resistant starch
Footnotes
[edit]- ^ a b c Eastwood M, Kritchevsky D (2005). "Dietary fiber: how did we get where we are?". Annu Rev Nutr. 25: 1–8. doi:10.1146/annurev.nutr.25.121304.131658. PMID 16011456.
- ^ a b c Anderson JW, Baird P, Davis RH; et al. (2009). "Health benefits of dietary fiber". Nutr Rev. 67 (4): 188–205. doi:10.1111/j.1753-4887.2009.00189.x. PMID 19335713.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ a b c d e f "Dietary Reference Intakes for Energy, Carbohydrate, fibre, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients) (2005), Chapter 7: Dietary, Functional and Total fibre" (PDF). US Department of Agriculture, National Agricultural Library and National Academy of Sciences, Institute of Medicine, Food and Nutrition Board.
- ^ Nugent, Anne P (2005). "Health properties of resistant starch". Nutrition Bulletin. 30 (1): 27–54. doi:10.1111/j.1467-3010.2005.00481.x.
- ^ Institute of Medicine; Food and Nutrition Board. Dietary Reference Intakes: energy, carbohydrates, fiber, fat, fatty acids, cholesterol, protein and amino acids. Washington (DC): National Academies Press; 2005.
- ^ American Association of Cereal Chemists. The definition of dietary fiber: report of the Dietary Fiber Definition Committee to the Board of Directors of the American Association of Cereal Chemists. Cereal Foods World. 2001;46:112–26.
- ^ Codex Alimentarius Commission; Food and Agriculture Organization; World Health Organization. Report of the 30th session of the Codex Committee on nutrition and foods for special dietary uses. ALINORM 9/32/26. 2009 [cited 2012 Mar 27]. Available from: http://www.codexalimentarius.net/download/report/710/al32_26e.pdf..
- ^ Fiber data derived from USDA National Nutrient Database for Standard Reference, Release 17.
- ^ Stacewicz-Sapuntzakis M, Bowen PE, Hussain EA, Damayanti-Wood BI, Farnsworth NR (May 2001). "Chemical composition and potential health effects of prunes: a functional food?". Crit Rev Food Sci Nutr. 41 (4): 251–86. doi:10.1080/20014091091814. PMID 11401245.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ http://www.webmd.com/vitamins-supplements/ingredientmono-205-Konjac+GLUCOMANNAN.aspx?activeIngredientId=205&activeIngredientName=Konjac+(GLUCOMANNAN)&source=2
- ^ Alvarado A, Pacheco-Delahaye E, Hevia P (2001). "Value of a tomato byproduct as a source of dietary fiber in rats" (PDF). Plant Foods Hum Nutr. 56 (4): 335–48. doi:10.1023/A:1011855316778. PMID 11678439.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Friedman G (September 1989). "Nutritional therapy of irritable bowel syndrome". Gastroenterol Clin North Am. 18 (3): 513–24. doi:10.1016/S0889-8553(21)00639-7. PMID 2553606.
- ^ Ewaschuk JB, Dieleman LA (October 2006). "Probiotics and prebiotics in chronic inflammatory bowel diseases". World J Gastroenterol. 12 (37): 5941–50. doi:10.3748/wjg.v12.i37.5941. PMC 4124400. PMID 17009391.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ Guarner F (April 2005). "Inulin and oligofructose: impact on intestinal diseases and disorders". Br J Nutr. 93 (Suppl 1): S61–5. doi:10.1079/BJN20041345. PMID 15877897.
- ^ Seidner DL, Lashner BA, Brzezinski A; et al. (April 2005). "An oral supplement enriched with fish oil, soluble fiber, and antioxidants for corticosteroid sparing in ulcerative colitis: a randomized, controlled trial". Clin Gastroenterol Hepatol. 3 (4): 358–69. doi:10.1016/S1542-3565(04)00672-X. PMID 15822041.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Rodríguez-Cabezas ME, Gálvez J, Camuesco D; et al. (October 2003). "Intestinal anti-inflammatory activity of dietary fiber (Plantago ovata seeds) in HLA-B27 transgenic rats". Clin Nutr. 22 (5): 463–71. doi:10.1016/S0261-5614(03)00045-1. PMID 14512034.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Ward PB, Young GP (1997). "Dynamics of Clostridium difficile infection. Control using diet". Adv Exp Med Biol. 412: 63–75. doi:10.1007/978-1-4899-1828-4_8. PMID 9191992.
- ^ Säemann MD, Böhmig GA, Zlabinger GJ (May 2002). "Short-chain fatty acids: bacterial mediators of a balanced host-microbial relationship in the human gut". Wien Klin Wochenschr. 114 (8–9): 289–300. PMID 12212362.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Cavaglieri CR, Nishiyama A, Fernandes LC, Curi R, Miles EA, Calder PC (August 2003). "Differential effects of short-chain fatty acids on proliferation and production of pro- and anti-inflammatory cytokines by cultured lymphocytes". Life Sciences. 73 (13): 1683–90. doi:10.1016/S0024-3205(03)00490-9. PMID 12875900.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ MacDermott RP (January 2007). "Treatment of irritable bowel syndrome in outpatients with inflammatory bowel disease using a food and beverage intolerance, food and beverage avoidance diet". Inflamm Bowel Dis. 13 (1): 91–6. doi:10.1002/ibd.20048. PMID 17206644.
- ^ Robertson, M. Denise; Wright JW; Loizon E; Debard C; Vidal H; Shojaee-Moradie F; Russell-Jones D; Umpleby AM (Epub ahead of print June 28, 2012). "Insulin-sensitizing effects on muswcle and adipose tissue after dietary fiber intake in men and women with metabolic syndrome". Journal of Clinical Endocrinology & Metabolism. 97 (9): 3326–32. doi:10.1210/jc.2012-1513. PMID 22745235.
{{cite journal}}: Check date values in:|date=(help) - ^ Kevin, Maki; Pelkman CL; Finocchiaro ET; Kelley KM; Lawless AL; Schild AL; Rains TM (April 2012). "Resistant starch from high-amylose maize increases insulin sensitivity in overweight and obese me". Journal of Nutrition. 142 (4): 717–723. doi:10.3945/jn.111.152975. PMC 3301990. PMID 22357745.
- ^ Johnston, KL; Thomas EL; Bell JD; Frost GS; Robertson MD (April 2010). "Resistant starch improves insulin sensitivity in metabolic syndrome". Diabetic Medicine. 27 (4): 391–397. doi:10.1111/j.1464-5491.2010.02923.x. PMID 20536509.
- ^ Phillips, Jodi (July 1995). "Effect of resistant starch on fecal bulk and fermentation-dependent events in humans". American Journal of Clinical Nutrition. 62 (1): 121–130. doi:10.1093/ajcn/62.1.121. PMID 7598054.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Ramakrishna, BS; Venkataraman S; Srinivasan P; Dash P; Young GP; Binder HJ (February 2000). "Amylase-resistant starch plus oral rehydration solution for cholera". The New England Journal of Medicine. 342 (5): 308–313. doi:10.1056/NEJM200002033420502. PMID 10655529.
- ^ Raghupathy, P; Ramakrishna BS; Oommen SP; Ahmed MS; Priyaa G; Dziura J; Young GP; Binder HJ (2006). "Amylase-resistant starch as adjunct to oral rehydration therapy in children with diarrhea". Journal of Pediatric Gastroenterology and Nutrition. 42 (4): 362–368. doi:10.1097/01.mpg.0000214163.83316.41. PMID 16641573.
- ^ Ramakrishna, Balakrishnan S.; Subramanian V; Mohan V; Sebastian BK; Young GP; Farthing MJ; Binder HJ (2008). "A randomized controlled trial of glucose versus amylase resistant starch hypo-osmolar oral rehydration solution for adult acute dehydrating diarrhea". PLOS ONE. 3 (2): e1587. doi:10.1371/journal.pone.0001587. PMID 18270575.
- ^ James, S. "P208. Abnormal fibre utilisation and gut transit in ulcerative colitis in remission: A potential new target for dietary intervention". Presentation at European Crohn's & Colitis Organization meeting, Feb 16-18, 2012 in Barcelona, Spain. European Crohn's & Colitis Organization. Retrieved 29 July 2012.
- ^ Kaur N, Gupta AK (December 2002). "Applications of inulin and oligofructose in health and nutrition" (PDF). J Biosci. 27 (7): 703–14. doi:10.1007/BF02708379. PMID 12571376.
- ^ Roberfroid MB (November 1, 2007). "Inulin-type fructans: functional food ingredients". J Nutr. 137 (11 Suppl): 2493S–2502S. doi:10.1093/jn/137.11.2493S. PMID 17951492.
- ^ Abrams S, Griffin I, Hawthorne K, Liang L, Gunn S, Darlington G, Ellis K (2005). "A combination of prebiotic short- and long-chain inulin-type fructans enhances calcium absorption and bone mineralization in young adolescents". Am J Clin Nutr. 82 (2): 471–6. doi:10.1093/ajcn.82.2.471. PMID 16087995.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Coudray C, Demigné C, Rayssiguier Y (2003). "Effects of dietary fibers on magnesium absorption in animals and humans". J Nutr. 133 (1): 1–4. doi:10.1093/jn/133.1.1. PMID 12514257.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Tako E, Glahn RP, Welch RM, Lei X, Yasuda K, Miller DD. (2007). "Dietary inulin affects the expression of intestinal enterocyte iron transporters, receptors and storage protein and alters the microbiota in the pig intestine". Br J Nutr. 99 (Sep): 1–9. doi:10.1017/S0007114507825128. PMID 17868492.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Parisi GC, Zilli M, Miani MP, Carrara M, Bottona E, Verdianelli G, Battaglia G, Desideri S, Faedo A, Marzolino C, Tonon A, Ermani M, Leandro G. (2002). "High-fiber diet supplementation in patients with irritable bowel syndrome (IBS): a multicenter, randomized, open trial comparison between wheat bran diet and partially hydrolyzed guar gum (PHGG)". Dig Dis Sci. 47 (8): 1697–704. doi:10.1023/A:1016419906546. PMID 12184518.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Gallaher, Daniel D. (2006). Dietary Fiber. Washington, D.C.: ILSI Press. pp. 102–110. ISBN 978-1-57881-199-1.
- ^ Weickert MO, Pfeiffer AF (2008). "Metabolic effects of dietary fiber consumption and prevention of diabetes". J Nutr. 138 (3): 439–42. doi:10.1093/jn/138.3.439. PMID 18287346.
- ^ Robertson, M. Denise; Currie JM; Morgan LM. Jewell DP; Frayn KN (2003). "Prior short-term consumption of resistant starch enhances postprandial insulin sensitivity in healthy subjects". Diabetologia. 46 (5): 659–665. doi:10.1007/s00125-003-1081-0. PMID 12712245.
- ^ Robertson, M. Denise; Bickerton AS; Dennis AL; Vidal H; Frayn KN (2005). "Insulin-sensitizing effects of dietary resistant starch and effects on skeletal muscle and adipose tissue metabolism". American Journal of Clinical Nutrition. 82 (3): 559–567. doi:10.1093/ajcn/82.3.559. PMID 16155268.
- ^ Zhang, Wen-qing; Wang Hong-wei; Zhang Yue-ming; Yang Yue-xin (March 2007). "Effects of resistant starch on insulin resistance of type 2 diabetes mellitus patients". Chinese Journal of Preventive Medicine. 2 (2): 101–104. PMID 17605234.
- ^ Johnston, KL; Thomas EL; Bell JD; Frost GS; Robertson MD (2010). "Resistant starch improves insulin sensitivity in metabolic syndrome". Diabetic Medicine. 27 (4): 391–397. doi:10.1111/j.1464-5491.2010.02923.x. PMID 20536509.
- ^ Maki, Kevin C.; Pelkman CL; Finocchiaro ET; Kelley KM; Lawless AL; Schild AL; Rains TM (April 2012). "Resistant starch from high-amylose maize increases insulin sensitivity in overweight and obese men". Journal of Nutrition. 142 (4): 717–723. doi:10.3945/jn.111.152975. PMC 3301990. PMID 22357745.
- ^ Robertson, M. Denise; Wright JW; Loizon E; Debard C; Vidal H; Shojaee-Moradie F; Russell-Jones D; Umpleby AM (June 28, 2012). "Insulin-sensitizing effects on muscle and adipose tissue after dietary fiber intake in men and women with metabolic syndrome". Journal of Clinical Endocrinology & Metabolism. 97 (9): 3326–32. doi:10.1210/jc.2012-1513. PMID 22745235.
- ^ "Dietary reference values for carbohydrates and dietary fiber". European Food Safety Authority.
- ^ Jones PJ, Varady KA (2008). "Are functional foods redefining nutritional requirements?" (PDF). Appl Physiol Nutr Metab. 33 (1): 118–23. doi:10.1139/H07-134. PMID 18347661.
- ^ Hermansson AM. Gel structure of food biopolymers In: Food Structure, its creation and evaluation.JMV Blanshard and JR Mitchell, eds. 1988 pp. 25-40Butterworths, London.
- ^ Rockland LB, Stewart GF. Water Activity: Influences on Food Quality. Academic Press, New York. 1991
- ^ Eastwood MA, Morris ER (1992). "Physical properties of dietary fibre that influence physiological function: a model for polymers along the gastrointestinal tract". Am J Clin Nutr. 55 (2): 436–442. doi:10.1093/ajcn/55.2.436.
- ^ Eastwood MA. The physiological effect of dietary fiber: an update.Annual Review Nutrition, 1992:12 : 19-35
- ^ Heaton KW, Marcus SN, Emmett PH, Bolton DH (1988). "Particle size of wheat, maize, oat test meals; effects on plasma glucose and insulin responses and rate of starch digestion in vitro". Am J Clin Nutr. 47 (4): 675–82. doi:10.1093/ajcn/47.4.675. PMID 2451416.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Jenkins DJA, Wolever TMS, Leeds AR; et al. (1978). "Dietary fibres, fibre analogues and glucose tolerance: importance of viscosity". Br Med J. 1 (6124): 1392–94. doi:10.1136/bmj.1.6124.1392. PMID 647304.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ a b c d Edwards CA, Johnson IT, Read NW. Do viscous polysaccharides reduce absorption by inhibiting diffusion or convection? Eur J Clin Nutr 1988;42:307-12.
- ^ a b Eastwood MA. The physiological effect of dietary fiber: an update.Annual Review Nutrition. 1992.12:19-35.
- ^ a b Carey MC, Small DM and Bliss CM. Lipid digestion and Absorption. Annual Review of Physiology. 1983.45:651-677.
- ^ Schneeman BO, Gallacher D. Effects of dietary fibre on digestive enzyme activity and bile acids in the small intestine. Proc Soc Exp Biol Med 1985; 180 409-14.
- ^ "Digestive tract in a horse".
- ^ Hellendoorn EW 1983 Fermentation as the principal cause of the physiological activity of indigestible food residue. In: Spiller GA (ed) Topics in dietary fiber research. Plenum Press, New York, pp 127-168
- ^ Brown L, Rosner B, Willett WW and Sacks FM (1999). "Cholesterol-lowering effects of dietary fiber: a meta-analysis". Amer J Clin Nutr. 69 (1): 30–42. doi:10.1093/ajcn/69.1.30. PMID 9925120.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Eastwood MA, Hamilton D (1968). "Studies on the adsorption of bile salts to non-absorbed components of diet". Biochim. Biophys. Act. 152: 159–166.
- ^ Gillissen and Eastwood; Eastwood, Martin A. (1995). "Taurocholic acid adsorption during non-starch polysaccharide fermentation: an in vitro study". British Journal of Nutrition. 74 (2): 221–227. doi:10.1079/BJN19950125. PMID 7547839.
- ^ Boerjan, Wout; Ralph, John; Baucher, Marie (2003). "Ligninbiosynthesis". Annual Review of Plant Biology. 54: 519–46. doi:10.1146/annurev.arplant.54.031902.134938. PMID 14503002.
- ^ "MedlinePlus Medical Encyclopedia: fiber". Retrieved 22 April 2009.
- ^ "University of MD Medical Center Encyclopedia entry for fiber". Retrieved 22 April 2009.
- ^ Gropper, Sareen S.; Jack L. Smith; James L. Groff (2008). Advanced nutrition and human metabolism (5th ed.). Cengage Learning. p. 114. ISBN 978-0-495-11657-8.
- ^ Food and Nutrition Board, Institute of Medicine of the National Academies (2005). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). National Academies Press. pp. 380–382.
- ^ Spiller, Gene; Margo N. Woods; Sherwood L. Gorbach (27 June 2001). Influence of fiber on the ecology of the intestinal flora. CRC Press. p. 257. ISBN 978-0-8493-2387-4. Retrieved 22 April 2009.
{{cite book}}:|work=ignored (help) - ^ Constantine Iosif Fotiadis; Christos Nikolaou Stoidis; Basileios Georgiou Spyropoulos; Eleftherios Dimitriou Zografos (November 14, 2008). "Role of probiotics, prebiotics and synbiotics in chemoprevention for colorectal cancer" (PDF). World Journal of Gastroenterology. 14. 14 (42). The WJG Press: 6454. doi:10.3748/wjg.14.6453. ISSN 1007-9327. Retrieved 22 April 2009.
{{cite journal}}: External link in|publisher= - ^ Greger JL (July 1999). "Nondigestible carbohydrates and mineral bioavailability". J Nutr. 129 (7 Suppl): 1434S–5S. doi:10.1093/jn/129.7.1434S. PMID 10395614.
- ^ Raschka L, Daniel H (November 2005). "Mechanisms underlying the effects of inulin-type fructans on calcium absorption in the large intestine of rats". Bone. 37 (5): 728–35. doi:10.1016/j.bone.2005.05.015. PMID 16126464.
- ^ Scholz-Ahrens KE, Schrezenmeir J (Nov 2007). "Inulin and oligofructose and mineral metabolism: the evidence from animal trials". J Nutr. 137 (11 Suppl): 2513S–2523S. doi:10.1093/jn/137.11.2513S. PMID 17951495.
- ^ a b Linus Pauling Institute at Oregon State University
- ^ Dietary fiber and whole-grain consumption in relation to colorectal cancer in the NIH-AARP Diet and Health Study, Arthur Schatzkin, Traci Mouw, etc, http://ajcn.nutrition.org/content/85/5/1353.full.pdf+html?sid=daf916fc-14c9-42c6-bd0f-d61335975d9b
- ^ Fuchs CS, Giovannucci EL, Colditz GA; et al. (January 1999). "Dietary fiber and the risk of colorectal cancer and adenoma in women". N Engl J Med. 340 (3): 169–76. doi:10.1056/NEJM199901213400301. PMID 9895396.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Simons CCJM; et al. (October 2010). "Bowel Movement and Constipation Frequencies and the Risk of Colorectal Cancer Among Men in the Netherlands Cohort Study on Diet and Cancer". Am J Epidemiol. 172 (12): 1404–14. doi:10.1093/aje/kwq307. PMID 20980354.
{{cite journal}}: Explicit use of et al. in:|author=(help) - ^ Britt Burton-Freeman, Amgen, Incorporated, Thousand Oaks, CA 91320-1799, Symposium: Dietary Composition and Obesity: Do We Need to Look beyond Dietary Fat?
- ^ fiber: Nutrition Source, Harvard School of Public Health
- ^ Dietary fibre. British Nutrition Foundation.
- ^ Lustig RH (December 2006). "The 'skinny' on childhood obesity: how our western environment starves kids' brains". Pediatr Ann. 35 (12): 898–902, 905–7. doi:10.3928/0090-4481-20061201-08. PMID 17236437.
- ^ Suter PM (2005). "Carbohydrates and dietary fiber". Handb Exp Pharmacol. Handbook of Experimental Pharmacology. 170 (170): 231–61. doi:10.1007/3-540-27661-0_8. ISBN 3-540-22569-2. PMID 16596802.[dead link]
- ^ U.S. Department of Agriculture; Agricultural Research Service. What we eat in America: nutrient intakes from food by gender and age. National Health and Nutrition Examination Survey (NHANES) 2007–2008 [cited 2012 Feb 20]. Available from: http://www.ars.usda.gov/SP2UserFiles/Place/12355000/pdf/0708/Table_1_NIN_GEN_07.pdf
- ^ Health claims: fruits, vegetables, and grain products that contain fiber, particularly soluble fiber, and risk of coronary heart disease. Electronic Code of Federal Regulations: US Government Printing Office, current as of October 20, 2008
- ^ Health claims: fiber-containing grain products, fruits, and vegetables and cancer. Electronic Code of Federal Regulations:US Government Printing Office, current as of October 20, 2008
- ^ a b c Tungland BC, Meyer D, Nondigestible oligo- and polysaccharides (dietary fiber): their physiology and role in human health and food, Comp Rev Food Sci Food Safety, 3:73-92, 2002 (Table 3)[1]
- ^ Venn BJ, Mann JI (November 2004). "Cereal grains, legumes and diabetes". Eur J Clin Nutr. 58 (11): 1443–61. doi:10.1038/sj.ejcn.1601995. PMID 15162131.
- ^ Lee YP, Puddey IB, Hodgson JM (April 2008). "Protein, fiber and blood pressure: potential benefit of legumes". Clin Exp Pharmacol Physiol. 35 (4): 473–6. doi:10.1111/j.1440-1681.2008.04899.x. PMID 18307744.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Theuwissen E, Mensink RP (May 2008). "Water-soluble dietary fibers and cardiovascular disease". Physiol. Behav. 94 (2): 285–92. doi:10.1016/j.physbeh.2008.01.001. PMID 18302966.
- ^ a b c WebMD Constipation
- ^ "Advisory letter concerning Docket No. FDA-2012-N-1210-0132 (see attached PDF)". regulations.gov. Food and Drug Administration. July 30, 2014. Retrieved August 22, 2014.
- ^ British Nutrition Foundation defines 'fibre'
- ^ a b British Nutrition Foundation
- ^ a b c FDA/CFSAN A Food Labeling Guide: Appendix C Health Claims, April 2008
- ^ Soluble Fiber from Certain Foods and Risk of Coronary Heart Disease, U.S. Government Printing Office, Electronic Code of Federal Regulations, Title 21: Food and Drugs, part 101: Food Labeling, Subpart E, Specific Requirements for Health Claims, 101.81 [2]
- ^ Park Y, Subar AF, Hollenbeck A, Schatzkin A (Feb 14, 2011). "Dietary fiber intake and mortality in the NIH-AARP Diet and Health Study". Arch Intern Med. 171 (12): 1061–8. doi:10.1001/archinternmed.2011.18. PMC 3513325. PMID 21321288.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ United Kingdom The Food Labelling Regulations 1996 – Schedule 7: Nutrition labelling
- ^ http://www.aaccnet.org/DietaryFiber/pdfs/dietfiber.pdf
- ^ a b Wong JM, de Souza R, Kendall CW, Emam A, Jenkins DJ (March 2006). "Colonic health: fermentation and short chain fatty acids". J Clin Gastroenterol. 40 (3): 235–43. doi:10.1097/00004836-200603000-00015. PMID 16633129.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Institute of Medicine (2005). Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington, D.C: National Academies Press. p. 347. ISBN 0-309-08525-X.
- ^ Drozdowski LA, Dixon WT, McBurney MI, Thomson AB (2002). "Short-chain fatty acids and total parenteral nutrition affect intestinal gene expression". J Parenter Enteral Nutr. 26 (3): 145–50. doi:10.1177/0148607102026003145. PMID 12005453.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Roy CC, Kien CL, Bouthillier L, Levy E (August 2006). "Short-chain fatty acids: ready for prime time?". Nutr Clin Pract. 21 (4): 351–66. doi:10.1177/0115426506021004351. PMID 16870803.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Scholz-Ahrens KE, Ade P, Marten B; et al. (March 1, 2007). "Prebiotics, probiotics, and synbiotics affect mineral absorption, bone mineral content, and bone structure". J Nutr. 137 (3 Suppl 2): 838S–46S. doi:10.1093/jn/137.3.838S. PMID 17311984.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link)
{kind=link}
{kind=link}
References
[edit]- Fiber, Harvard School of Public Health
- Fiber Health Claims That Meet Significant Scientific Agreement, US Food and Drug Administration
- Higgins JA (2004). "Resistant starch: metabolic effects and potential health benefits". J AOAC Int. 87 (3): 761–8. doi:10.1093/jaoac/87.3.761. PMID 15287677.
- Tungland BC, Meyer D. Nondigestible oligo- and polysaccharides (dietary fiber): their physiology and role in human health and food. Comprehensive Reviews in Food Science and Food Safety 1:73-92, 2002.
- Parisi GC, Zilli M, Miani MP; et al. (August 2002). "High-fiber diet supplementation in patients with irritable bowel syndrome (IBS): a multicenter, randomized, open trial comparison between wheat bran diet and partially hydrolyzed guar gum (PHGG)" (PDF). Dig Dis Sci. 47 (8): 1697–704. doi:10.1023/A:1016419906546. PMID 12184518.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - Marlett JA (2001). "Dietary fiber and cardiovascular disease". In Dreher ML, Cho SS (ed.). Handbook of dietary fiber. New York: M. Dekker. pp. 17–30. ISBN 0-8247-8960-1.
- US Food and Drug Administration. Health Claims: Soluble fiber from certain foods and risk of heart diseases. Code of Federal Regulations. 2001;21:101.81.
- Eastwood MA, Brydon WG, Tadesse K (1980). "Effect of fiber on colon function". In Kay R, Spiller GA (ed.). Medical aspects of dietary fiber. New York: Plenum Medical Book Co. pp. 1–26. ISBN 0-306-40507-5.
{{cite book}}: CS1 maint: multiple names: authors list (link) - Prynne CJ, Southgate DA (May 1979). "The effects of a supplement of dietary fiber on faecal excretion by human subjects". Br J Nutr. 41 (3): 495–503. doi:10.1079/BJN19790064. PMID 465439.
- National Nutrient Database at USDA Website
External links
[edit]- Food Sources of Dietary Fiber, Appendix B-8, Dietary Guidelines for Americans published jointly in 2005 by the US Department of Health and Human Services and the Department of Agriculture
- Anatomy and Function of the Human Digestive System