
Talk:Treatment and management of COVID-19
| This is the talk page for discussing improvements to the Treatment and management of COVID-19 article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find medical sources: Source guidelines · PubMed · Cochrane · DOAJ · Gale · OpenMD · ScienceDirect · Springer · Trip · Wiley · TWL |
| This article is rated C-class on Wikipedia's content assessment scale. It is of interest to the following WikiProjects: | |||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||
.svg)


| The contentious topics procedure applies to this page. This page is related to COVID-19, broadly construed, which has been designated as a contentious topic. Editors who repeatedly or seriously fail to adhere to the purpose of Wikipedia, any expected standards of behaviour, or any normal editorial process may be blocked or restricted by an administrator. Editors are advised to familiarise themselves with the contentious topics procedures before editing this page. |
Wiki Education Foundation-supported course assignment
[edit]![]() This article was the subject of a Wiki Education Foundation-supported course assignment, between 14 July 2020 and 28 August 2020. Further details are available on the course page. Student editor(s): WilliamWang002.
This article was the subject of a Wiki Education Foundation-supported course assignment, between 14 July 2020 and 28 August 2020. Further details are available on the course page. Student editor(s): WilliamWang002.
Above undated message substituted from Template:Dashboard.wikiedu.org assignment by PrimeBOT (talk) 04:26, 18 January 2022 (UTC)
Mechanical ventilation claim
[edit]"a percentage of cases are in need of mechanical ventilation" seems to me pretty vague. Can we put a percentage range, or even a likelihood statement (i.e. very likely, likely), as it stands it could mean anything, really. Forich (talk) 20:43, 30 April 2021 (UTC)
Orphaned references in Management of COVID-19
[edit]I check pages listed in Category:Pages with incorrect ref formatting to try to fix reference errors. One of the things I do is look for content for orphaned references in wikilinked articles. I have found content for some of Management of COVID-19's orphans, the problem is that I found more than one version. I can't determine which (if any) is correct for this article, so I am asking for a sentient editor to look it over and copy the correct ref content into this article.
Reference named "WHO2020QA":
- From Coronavirus disease 2019: "Q&A on coronaviruses (COVID-19)". World Health Organization (WHO). 17 April 2020. Archived from the original on 14 May 2020. Retrieved 14 May 2020.
- From Severe acute respiratory syndrome coronavirus 2: "Q&A on coronaviruses (COVID-19)". World Health Organization (WHO). 11 February 2020. Archived from the original on 20 January 2020. Retrieved 24 February 2020.
- From COVID-19 pandemic in South Asia: "Q&A on coronaviruses". WHO.int. World Health Organization. 11 February 2020. Retrieved 24 February 2020.
- From COVID-19 pandemic in Nepal: "Q&A on coronaviruses". WHO.int. World Health Organization. 11 February 2020. Archived from the original on 20 January 2020. Retrieved 24 February 2020.
I apologize if any of the above are effectively identical; I am just a simple computer program, so I can't determine whether minor differences are significant or not. AnomieBOT⚡ 01:56, 2 June 2020 (UTC)
Orphaned references in Management of COVID-19
[edit]I check pages listed in Category:Pages with incorrect ref formatting to try to fix reference errors. One of the things I do is look for content for orphaned references in wikilinked articles. I have found content for some of Management of COVID-19's orphans, the problem is that I found more than one version. I can't determine which (if any) is correct for this article, so I am asking for a sentient editor to look it over and copy the correct ref content into this article.
Reference named "Lancet2020Flatten":
- From COVID-19 pandemic: Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD (March 2020). "How will country-based mitigation measures influence the course of the COVID-19 epidemic?". Lancet. 395 (10228): 931–934. doi:10.1016/S0140-6736(20)30567-5. PMC 7158572. PMID 32164834.
A key issue for epidemiologists is helping policy makers decide the main objectives of mitigation—e.g. minimising morbidity and associated mortality, avoiding an epidemic peak that overwhelms health-care services, keeping the effects on the economy within manageable levels, and flattening the epidemic curve to wait for vaccine development and manufacture on scale and antiviral drug therapies.
- From Coronavirus disease 2019: Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD (March 2020). "How will country-based mitigation measures influence the course of the COVID-19 epidemic?". Lancet. 395 (10228): 931–934. doi:10.1016/S0140-6736(20)30567-5. PMC 7158572. PMID 32164834.
A key issue for epidemiologists is helping policy makers decide the main objectives of mitigation—e.g. minimising morbidity and associated mortality, avoiding an epidemic peak that overwhelms health-care services, keeping the effects on the economy within manageable levels, and flattening the epidemic curve to wait for vaccine development and manufacture on scale and antiviral drug therapies.
I apologize if any of the above are effectively identical; I am just a simple computer program, so I can't determine whether minor differences are significant or not. AnomieBOT⚡ 22:55, 1 August 2020 (UTC)
Secondary source on the efficacy of inexpensive steroids in treating COVID-19
[edit]Can someone weave in this secondary source on cheap steroids to treat severe Covid?
- The WHO Rapid Evidence Appraisal; Sterne, Jonathan A. C.; Murthy, Srinivas; Diaz, Janet V.; et al. (2020-09-02). "Association Between Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19". JAMA. doi:10.1001/jama.2020.17023. Retrieved 2020-09-02.
News source:
- Gallagher, James (2020-09-02). "Cheap steroids save lives from severe Covid". BBC News. Retrieved 2020-09-02.
Peaceray (talk) 17:04, 2 September 2020 (UTC)
Large pool of references to mine.
[edit]In this selection of BMJ Rapid Responses to a subscribers only question, there are a number of well reasoned responses, including one one by Robert A Brown with 86 very well selected references relating to the connection between Vitamin-D and CoViD-19.
I suggest anyone with the patience to dig through them might find a lot of useful material for fleshing out the somewhat feeble Vitamin-D section.
I decline to edit this article as I would possibly loose my calm.
From the British Medical Journal we have Sixty seconds on . . . vitamin D
Idyllic press (talk) 21:08, 23 October 2020 (UTC)
Treatment and management of COVID-19
[edit]Any objections to changing the title to 'Treatment and management of COVID-19'? Now that treatment content is located here instead of in Coronavirus disease 2019 and there are actual treatments available, it seems like a better title for the page. - Wikmoz (talk) 21:40, 3 December 2020 (UTC)
- @Gtoffoletto, Tenryuu, Moxy, Bakkster Man, Ovinus Real, Sdkb, RealFakeKim, and Doc James: Any thoughts on this? In addition to the above, "treatment" is the more recognizable term for the general public seeking this information. - Wikmoz (talk) 21:43, 3 December 2020 (UTC)
- Sounds fine to me. {{u|Sdkb}} talk 21:48, 3 December 2020 (UTC)
- Wikmoz, seeing as treatment is a big part of management, I think that makes sense. For MoS purposes, "management" should be decapitalised for sentence style if this goes through. —Tenryuu 🐲 ( 💬 • 📝 ) 21:52, 3 December 2020 (UTC)
- Ah! Good catch! I've fixed the proposal accordingly. - Wikmoz (talk) 21:54, 3 December 2020 (UTC)
 Like--Moxy 🍁 02:45, 4 December 2020 (UTC)
Like--Moxy 🍁 02:45, 4 December 2020 (UTC)- Like I agree management seems too narrow in terms of scope for the article. Once this is done we should really improve the lead though as it doesn't cover treatment sufficiently at the moment and since it is transcluded into the main article it leaves a big gap in content. -- {{u|Gtoffoletto}} talk 09:36, 4 December 2020 (UTC)
- Agreed. I'll try adding a notice. - Wikmoz (talk) 19:29, 4 December 2020 (UTC)
- Support - Good update. Even if existing treatments are of marginal effectiveness (depending who you ask), it still makes sense as a title. Bakkster Man (talk) 14:49, 4 December 2020 (UTC)
First meta-analysis of the effect of Ivermectin on Covid 19 patients
[edit]Can I suggest including a summary of the first meta-analysis of Ivermectin's effect on Covid 19 patients? I suggest:
"The first meta-analysis of Ivermectin's effect on Covid 19 patients found a modest utility of Ivermectin in reducing all-cause mortality and improving clinical outcomes" [[1]] The reduction in mortality was actually 47% ( rising to 50% if a late-arriving addition study was included,) but the quality of evidence was very low. However, the results are backed up by 28 other studies, all of which saw a strong improvement in clinical outcomes, including an overall average 82% reduction in mortality [[2]] AussiePete56 (talk) 01:25, 31 December 2020 (UTC)
- As you've been told at Ivermectin, this would be a problematic POV skewing of the source. As we know from RS Ivermectin has become the latest drug to be pushed as a "miracle cure" in the crank-o-sphere, but the research support for there being benefit is weak, where not based on fraudulent data (the Surgisphere debacle[3]). This is detailed at Ivermectin#COVID-19, and anything we say here should be in sync with that. Alexbrn (talk) 01:35, 31 December 2020 (UTC)
The suggested summary is a direct quote from the "Conclusion" paragraph in the study, so to call it a "problematic POV skewing of the source" is preposterous. This "modest utility" version of a summary was my compromise since you objected to mentioning the "47% reduction in mortality" as part of the summary - it is this 47% figure that you called "a problematic skewing of the source", not the "modest utility" version. As of the time of writing this, you have not responded at all on the Ivermectin page to this compromise suggestion. I'm starting to lose count of these kinds of mistakes you're making.
Again you insist on down-playing effectiveness and emphasising unreliability of this meta-analysis. I'm not suggesting that the 28 other studies be included on Wikipedia, but the authors of that article have calculated that the chances of Ivermectin actually having a nil benefit, taking the 28 studies as a whole, is one in 268 million. You are going "all-in" on that "one". Ridiculous. AussiePete56 (talk) 02:07, 31 December 2020 (UTC)
- Yeah, you have made up another figure now: 82%. Alexbrn (talk) 02:10, 31 December 2020 (UTC)
Of the 28 studies, twelve focused specifically on mortality - of these twelve, the overall average improvement was 82% (see figure 7). Another mistake. AussiePete56 (talk) 02:19, 31 December 2020 (UTC)
- Wikipedia reflects reliable sources, not editors' novel reinterpretation of the primary data in ways the source does not do itself. The article[4] has no "figure 7" (Add: Oh I see you're using the "fake" journal article at ivmmeta.com ... we're obviously not going to be citing that!) Alexbrn (talk) 02:36, 31 December 2020 (UTC)
As I said, I'm not suggesting using the collation of the 28 studies (ten of which are Randomised Control Studies - average improvement using Ivermectin - 78%) on the main page, but it can be mentioned on the talk page to help make a point. The reported benefit from this meta-analysis is actually more modest than the 28 studies taken together, is the point.
So can I suggest a couple of options - "The first meta-analysis of Ivermectin's effect on Covid 19 patients supports recent observational studies which have reported the effectiveness of this drug as add-on therapy in patients with COVID-19, and suggests the modest utility of ivermectin in reducing all-cause mortality and improving clinical outcomes." [[5]] (This is a direct quote from its "Conclusions") or, more simply, "The first meta-analysis of Ivermectin's effect on Covid 19 patients suggests a modest utility of Ivermectin in reducing all-cause mortality and improving clinical outcomes" [[6]] AussiePete56 (talk) 03:25, 31 December 2020 (UTC)
- I don't know why you're linking to fake research papers then. For the RS, Wikipedia is meant to summarize, and cherry-picked copy 'n' pasting risks WP:COPYVIO. You excerpt misrepresents the source because it omits to account for the extensive discussion in the source of the very low quality of the evidence. This has been discussed at Ivermectin at length and whatever we have here, should be in sync with what is there. As far as actual clinical guidance goes, the NIH recommendation is not to use Ivermectin; that is most pertinent to this article. Alexbrn (talk) 03:41, 31 December 2020 (UTC)
So the 28 research papers are not just unreliable, Alexbrn declares them all to be actually "fake" - without evidence.
Regarding copyright violations - the publisher of the study is The Journal of Pharmacy and Pharmaceutical Sciences - its the official journal of the Canadian Society for Pharmaceutical Sciences. They state that, "This is an open-access article distributed under the terms of the Creative Commons License (Attribution-ShareAlike 4.0 International), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited."
You say that my cut-and-paste of their Conclusion misrepresents the article because it omits to account for the extensive discussion in the source of the very low quality of the evidence. The authors' choice of what to say in their Conclusion obviously takes into account EVERY aspect of the study, including the quality of the evidence. As someone with little or no medical training yourself (I assume - certainly less than the authors of the study) it is preposterous for an unqualified layman like yourself to tell the experts that they have made a mistake in the choice of words they have used in their conclusion. Since Wikipedia is supposed to "summarise" the source we're linking to, what could be more obvious, accurate or simple than to just use the summary conclusion that the expert authors themselves have helpfully provided?
Regarding being in sync with the "Ivermectin" page - you shut down further discussion there, not because the matter was resolved, but because you were losing every argument, and you wanted it to stop.
Regarding the NIH recommendation, as Professor Kory pointed out in his Senate testimony, the NIH issued that recommendation in August 2020 - well before the vast majority of the research in favour of Ivermectin was released. In any event, why do you take the trouble to even mention this, except as more evidence of a non NPOV? We are just discussing how to best summarise the article, what has the NIH got to do with it? AussiePete56 (talk) 03:23, 1 January 2021 (UTC)
- Probably better to WP:FOC rather than WP:BATTLE and re-prove Danth's Law again.
- Editors have an obligation to read and summarize whole sources for a lay audience in a way consistent with MOS:MED, not just cherry pick excerpts in service of a POV. One might as well "pick" the excerpt: "Definitive evidence for repurposing this drug for COVID-19 patients will emerge only in the future". And leave it at that. What we currently have at Ivermectin is fair and good.
- A clinical guideline is cited at Ivermectin because they are the best type of sources per WP:MEDASSESS.
- I notice the twitter account of the anonymous people pushing the fake article you link has now been suspended; this is the opposite of the kind of source Wikipedia wants. I have added ivermectin to this article consistent with the way other unapproved-but-under-research drugs are dealt with here, in a way which satisfied WP:V. I shall not respond further unless/until new good sourcing emerges. Alexbrn (talk) 09:52, 1 January 2021 (UTC)
So you're citing Twitter now as a judge of medical qualifications? Wow. Even distinguished Professor Pierre Kory, author of hundreds of published, peer-reviewed studies and Chief of Critical Care at his hospital, had a Facebook post deleted recently because it didn't reflect the official policy that there is no effective treatment option for severe Covid patients except for ventilation. He's on the frontline, saving patients' lives every day, and achieved a remarkable reduction in his hospital's fatality rate from 23% to 6%, but Facebook sees fakes and frauds everywhere, like hypervigilant Wikipedia editors.... AussiePete56 (talk) 15:50, 2 January 2021 (UTC)
- This is WP:NOTAFORUM. The pertinent point here is this is the opposite of the kind of source Wikipedia wants, as content must be WP:Verified by WP:Reliable sources, which are characterized by "a reputation for fact checking and accuracy". Getting banned from social media platforms even further confirms the lack of such a reputation in this instance. Is there any reliable secondary coverage on how Facebook is cracking down on ivermectin misinformation? That might be of some use to Wikipedia. Alexbrn (talk) 16:05, 2 January 2021 (UTC)
"Is there any reliable secondary coverage of how Facebook makes decisions on medical matters" Lol . Perhaps you should make some enquiries about the practices of Instagram and TikTok while you're at it.
How about this addition to the "Convalescent plasma" section of "Experimental Treatments"?
"In December 2020 the Central American country of Belize announced that it had begun using convalescent plasma and Ivermectin to treat patients of Covid 19 with severe symptoms. [[7]] — Preceding unsigned comment added by AussiePete56 (talk • contribs) 06:14, 4 January 2021 (UTC)
To please Alexbrn even more, I even found a Facebook report on this development... [[8]] AussiePete56 (talk) 06:16, 4 January 2021 (UTC)
- "As far as actual clinical guidance goes, the NIH recommendation is not to use Ivermectin; that is most pertinent to this article." Alexbrn
- I don't know if it is wise to use the NIH as a reliable source if there are other similar sources with the opposite viewpoint. Remember just because this is the English language Wikipedia it should not be construed to be England centric.
- "The implementation of such policies kicked off on 8 May, when the Peruvian Ministry of Health recommended using ivermectin to treat mild and severe cases of COVID-19. Days later, Bolivia’s government added the drug to its guidelines for treating coronavirus infections. The municipality of Natal, in Rio Grande Do Norte, Brazil, also promoted it as a preventative — to be taken by health-care professionals and people at increased risk of severe illness from the virus, because of “its safe pharmacological profile, clinical experience using it against other diseases, cost and dosage convenience”."
- Even if we do not put Ivermectin front and centre on the page I think it would be prudent for people to be kind to each other and keep an open mind on the talk page.
- Idyllic press (talk) 21:46, 17 January 2021 (UTC)
- I agree that some WP:WORLDVIEW fixes are in order. I have added some information from Brazil and Peru, arguably the countries where ivermectin use for COVID-19 is most widespread. (However, I have done so at the corresponding section of COVID-19 drug repurposing research, not this article.) Fvasconcellos (t·c) 07:18, 18 January 2021 (UTC)
Does the USFDA consider monoclonal antibodies to be more effective/safe than Ivermectin?
[edit]Fvasconcellos wrote in the article history: "we have been over this time and again. this is an inappropriate synthesis and is inaccurate. The monoclonal antibodies have been granted EUA status; ivermectin has *not* "
The editor asserts that the EUA from the FDA should be interpreted to mean monoclonal antibodies for COVID-19 is superior to Ivermectin which received standard USFDA approval. The editor needs to provide a reference that is supportive. Editor opinion is meaningless. The evidence to the contrary is from the Front Line COVID-19 Critical Care Alliance who advised the NIH on their decision.--Vrtlsclpl (talk) 17:46, 18 January 2021 (UTC)
- Is there an actual edit proposed? Alexbrn (talk) 17:54, 18 January 2021 (UTC)
- There is no interpretation of superiority. The sentence introduced by your edit—
Ivermectin now holds the same approval and recommendation status for COVID-19 as bamlanivimab and casirivimab-imdevimab, in the view of U.S. health authorities
—is simply inaccurate. The two monoclonal antibodies have been authorized for emergency use in COVID-19, as a result of evidence from clinical trials. Ivermectin has not been authorized or approved for such use. You are conflating FDA approval and NIH recommendation. It is an inappropriate and inaccurate synthesis of the current situation. Also, a press release from the "Front Line COVID-19 Critical Care Alliance" is neither evidence nor a reliable source. Fvasconcellos (t·c) 18:21, 18 January 2021 (UTC)
- There is no interpretation of superiority. The sentence introduced by your edit—
Is this MEDRS? Apologies if not... https://www.medscape.com/viewarticle/944440--Sloorbeadle (talk) 05:27, 30 January 2021 (UTC)
Nitric oxide
[edit]I found one (I believe to be WP:MEDRS) source regarding nitric oxide with COVID-19 treatment.[1]
Specifically, "In mechanically ventilated adults with COVID-19 ARDS, we recommend against the routine use of inhaled nitric oxide (strong recommendation, low-quality evidence)" and related content (next paragraph from source).
Given this, I'd support adding some content either here (or perhaps better at COVID-19 drug repurposing research) that clearly indicates nitric oxide is not recommended with rationale summary. Jdphenix (talk) 18:07, 22 January 2021 (UTC)
References
- ^ Alhazzani, Waleed; Møller, Morten Hylander; Arabi, Yaseen M.; Loeb, Mark; Gong, Michelle Ng; Fan, Eddy; Oczkowski, Simon; Levy, Mitchell M.; Derde, Lennie; Dzierba, Amy; Du, Bin; Aboodi, Michael; Wunsch, Hannah; Cecconi, Maurizio; Koh, Younsuck; Chertow, Daniel S.; Maitland, Kathryn; Alshamsi, Fayez; Belley-Cote, Emilie; Greco, Massimiliano; Laundy, Matthew; Morgan, Jill S.; Kesecioglu, Jozef; McGeer, Allison; Mermel, Leonard; Mammen, Manoj J.; Alexander, Paul E.; Arrington, Amy; Centofanti, John E.; Citerio, Giuseppe; Baw, Bandar; Memish, Ziad A.; Hammond, Naomi; Hayden, Frederick G.; Evans, Laura; Rhodes, Andrew (21 April 2020). "Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19)". Critical Care Medicine. doi:10.1097/CCM.0000000000004363. Retrieved 22 January 2021.
As I said earlier, sticking to primary sources during a pandemic makes lttle sense since events are changing so rapidly. In any case here are two sources on nitric oxide that would seem to qualify for MEDRS approval:
British Medical Association Best Practices Article: https://bestpractice.bmj.com/topics/en-gb/3000201/emergingtxs
And a review article: The Potential Role of Inhaled Nitric Oxide in Managing COVID-19 Associated Lung Complications Review of Literature https://clinmedjournals.org/articles/ijrpm/international-journal-of-respiratory-and-pulmonary-medicine-ijrpm-7-145.php?jid=ijrpm
Cari.Firelight (talk) 06:22, 24 January 2021 (UTC)
- That review article's in a predatory journal. Jdphenix' source is good. Alexbrn (talk) 07:36, 24 January 2021 (UTC)
Nitric oxide deserves a mention. There are numerous studies in-flight in the US alone (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7328337/#!po=2.77778)
And while they do recommend against the use of NO in mechanically ventilated patients, that doesn't preclude it from being studied in other stages of the disease. Sloorbeadle (talk) 06:59, 25 January 2021 (UTC)
- Note: The main article for nitric oxide + COVID currently appears to be Biological functions of nitric oxide#COVID-19.
- This article (Treatment and management of COVID-19) may not be the best fit, because dozens of drugs and treatments are being researched for possible COVID-19 use. See COVID-19 drug repurposing research and COVID-19 drug development. We don't necessarily want to give a lot of WP:WEIGHT to one of these dozens of candidates by talking about it too much in this article.
- I'm not 100% sure how to handle this yet, but maybe a section in COVID-19 drug repurposing research would be a good spot for it. –Novem Linguae (talk) 07:22, 25 January 2021 (UTC)
 Done I ended up adding something here, because Jdphenix's (good) source was a practice guideline, so this is something which is actively recommended against in practice, rather than (just) something being investigated. Alexbrn (talk) 13:43, 26 January 2021 (UTC)
Done I ended up adding something here, because Jdphenix's (good) source was a practice guideline, so this is something which is actively recommended against in practice, rather than (just) something being investigated. Alexbrn (talk) 13:43, 26 January 2021 (UTC)
Ivermectin, different aspect
[edit]The who says people are dying because they're not taking ivermectin when they have covid and are put on corticosteroids. The who. Like the ultimate authority if ever there was one. They set practice for most of the world.
This is some bullshit.
What the hell is disruptive about adding this to the article?
| “ | The WHO states ivermectin use is "advisable" when steroids are used, including for COVID-19, as presumptive treatment where there is a high or moderate risk of a parasite hyperinfection side effect from the steroid. [1] This applies to perhaps half the world's population. | ” |
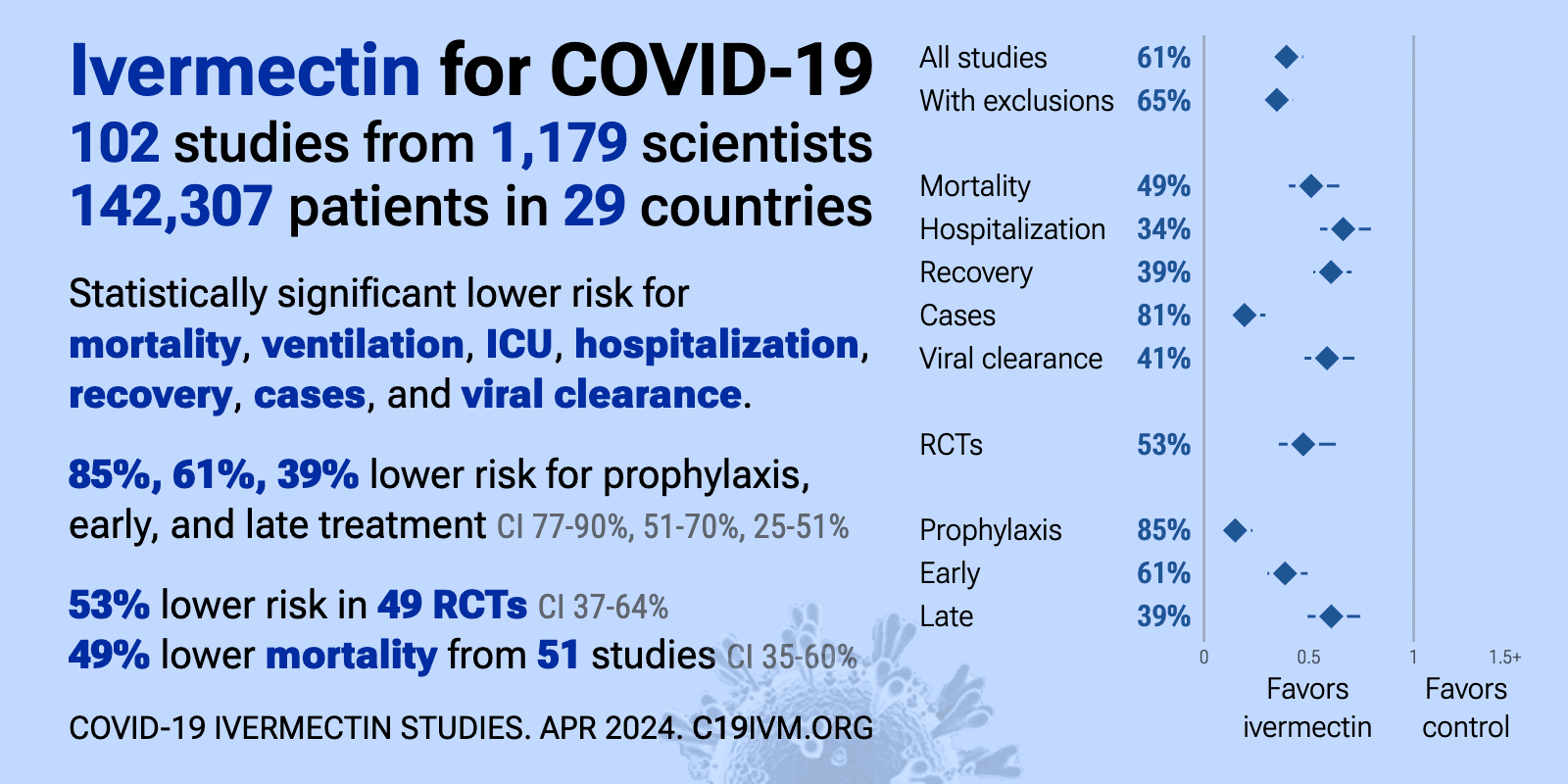
FYI: Ivermectin stops covid - according to people who aren't ignorant, that is. Per https://c19ivermectin.com/isummary.png
{kind=link}
Those who "were born, resided, or had long-term travel in
- High RISK: Southeast Asia, Oceania, sub-Saharan Africa, South America, or the Caribbean."
- risk moderate :Central America, Eastern Europe, Mediterranean, Mexico, Middle East, North Africa, Indian sub-continent, or Asia."
What a coincidence - the areas where ivermectin is considered unnecessary include many of the ones with the highest covid mortality rates = Australia, Canada, United States, and Western Europe). --50.201.195.170 (talk) 10:15, 25 January 2021 (UTC)
 Not done
Not done Partly done The source does mention COVID-19 however, so have added this in such a way that WP:V should be satisfied. Also added something at Strongyloidiasis. Alexbrn (talk) 13:46, 26 January 2021 (UTC)
Partly done The source does mention COVID-19 however, so have added this in such a way that WP:V should be satisfied. Also added something at Strongyloidiasis. Alexbrn (talk) 13:46, 26 January 2021 (UTC)
Why are you still casting aspersions on my edit? Again, how did my edit here - https://en.wikipedia.org/w/index.php?diff=1002626197 - not satisfy V or qualify as disruptive? You complained about it and got me blocked over it. Deleting my addition was extremely aggressive, but I got blocked for asking a question, which you took offense to. I've apologized, but do you now think perhaps you overreacted? Since you've somewhat restored my edit, which I'm happy to see, and used the same main source, which made my original edit so easily verifiable? (No one has even attempted to show otherwise.) --50.201.195.170 (talk) 21:53, 13 February 2021 (UTC)
Was censoring my post here (which remains censored) really necessary? Given that it broke rules about not editing others comments, it seems pretty extraordinary. --50.201.195.170 (talk) 21:09, 13 February 2021 (UTC)
New treatments with sources
[edit]The following may be relevant, or may become relevant. If considered acceptable they can be added now.
- === EXO-CD24 ===
In February 2021 the drug EXO-CD24[1] in a stage 1 clinical trial[2] showed significant positive outcomes on moderate-to-severe cases of Covid19 infections. The drug is based on exosomes used by the body for intercellular communication, enriched with CD24 protein expressed on the surface of the cell. It is delivered by one inhalation session daily for five days, and inhibits the over-secretion of cytokines.
- ^ Abigail Klein Leichman (7 February 2021). "Has Israel just found the cure for Covid?". Israel21c.
- ^ "Evaluation of the Safety of CD24-Exosomes in Patients With COVID-19 Infection". ClinicalTrials.gov. 10 February 2021. Retrieved 10 February 2021.
{{cite web}}: CS1 maint: url-status (link)
- ===Inhaled budesonide===
The Stoic study[1] was a response to observing that surprisingly few people with asthma or chronic obstructive pulmonary disease (COPD) were admitted to hospital with Covid-19, although other respiratory illnesses tend to worsen outcomes. The possibility that steroid inhalers used to manage asthma and COPD symptoms were protective against severe Covid-19 was investigated at the University of Oxford. Half of a sample of 146 patients with early Covid-19 symptoms received 800 micrograms of budesonide twice a day until they felt better; one of the patients who inhaled budesonide needed hospital intervention, while ten of the control group did. The budesonide group experienced a faster resolution of fever and other Covid-19 symptoms, and had fewer persistent symptoms after 28 days. It has been suggested that the drug reduces inflammatory damage caused by the immune response, or it may reduce viral replication in these cells, or make it harder for the virus to attach to them.[2][3]
As of February 2021[update] at least five other studies were being carried out into different classes of inhaled corticosteroids. The Principle trial,[4] also led by Oxford researchers, is evaluating budesonide as a treatment for older adults with early Covid-19 symptoms, including those with underlying health conditions.
James Dodd of North Bristol Lung Centre and the University of Bristol said: "If that level of efficacy is reproduced in a larger study, including older age groups with other comorbidities, you really have got potentially a very exciting, cheap, safe, widely available treatment for patients in the community who have just been diagnosed with Covid-19".[3]
- ^ "About STOIC study". STOIC Study - University of Oxford. Retrieved 13 February 2021.
- ^ Ramakrishnan, Sanjay; Nicolau, Dan V.; Langford, Beverly; Mahdi, Mahdi; Jeffers, Helen; Mwasuku, Christine; Krassowska, Karolina; Fox, Robin; Binnian, Ian; Glover, Victoria; Bright, Stephen; Butler, Christopher; Cane, Jennifer L; Halner, Andreas; Matthews, Philippa C; Donnelly, Louise E; Simpson, Jodie L; Baker, Jonathan R; Fadai, Nabil T; Peterson, Stefan; Bengtsson, Thomas; Barnes, Peter J; Russell, Richard EK; Bafadhel, Mona (8 February 2021). "Inhaled budesonide in the treatment of early COVID-19 illness: a randomised controlled trial". medRxiv - The preprint server for health services. doi:10.1101/2021.02.04.21251134.
- ^ a b Geddes, Linda (10 February 2021). "Asthma drug may reduce risk of severe Covid if taken early – study". The Guardian.
- ^ "Join the PRINCIPLE Trial". PRINCIPLE - Platform Randomised trial of INterventions against COVID-19 In older peoPLE. Retrieved 13 February 2021.
Best wishes, Pol098 (talk) 21:05, 13 February 2021 (UTC)
Extended-confirmed-protected edit request on 26 February 2021
[edit]This edit request has been answered. Set the |answered= or |ans= parameter to no to reactivate your request. |
I would like to add the results of this new article:
TRIM56, a member of the fifth group subfamily of TRIM proteins, is a cytoplasmic protein. It may exert direct antiviral effects against distinct positive- and negative-sense, single-stranded RNA viruses. TRIM56 may be a feasible candidate in the management of the medically notable viral pathogens particularly, COVID-19. https://www.tandfonline.com/doi/full/10.1080/1744666X.2020.1822168 Maryhook97 (talk) 03:38, 26 February 2021 (UTC)
- Not done It is a long way from "may exert direct antiviral effects" to human clinical trials and even farther to treatment and management which is the focus of this article. There were only two studies in the review that had any in vivo components. It is far too preliminary. BiologicalMe (talk) 15:27, 26 February 2021 (UTC)
Extended-confirmed-protected edit request on 15 March 2021
[edit]This edit request has been answered. Set the |answered= or |ans= parameter to no to reactivate your request. |
CHANGE FROM:
Several potentially disease-modifying treatments have been investigated and found to be ineffective or unsafe, and are thus not recommended for use; these include baloxavir marboxil, favipiravir, lopinavir/ritonavir, ruxolitinib, chloroquine, hydroxychloroquine, interferon β-1a, and colchicine.[13]
CHANGE TO:
Several potentially disease-modifying treatments have been investigated. Some have been found to be ineffective, unsafe, or have limited research data; these include baloxavir marboxil, favipiravir, lopinavir/ritonavir, ruxolitinib, chloroquine. Some are used in some countries but not others as there is disputed data from international sources, thus not recommended for use in some countries as has been seen with the disputed use of hydroxychloroquine [9]. Sme have been found to be effective and providing hope for early treatment which is a critical gap in the treatment at this time; these include Colchicine [10] and Ivermectin [11]. Ivemectin is now the most studied of all potential early interventions treatment for COVID-19 with 71 studies, 34 peer reviewed, 46 with results comparing treatment and control groups. Evamigdal (talk) 09:55, 15 March 2021 (UTC)
- Not done The proposed modification is based on unreliable sources. Alexbrn (talk) 10:21, 15 March 2021 (UTC)
Disordered list?
[edit]The article currently enumerates the treatments in a disordered matter, I fail to see any sorting of the information, whether chronological, by weight-of-evidence, by intensity-of-results, by nature of treatment, or any other order. The treatments seems to jump around throughout the sections. I propose we discuss here a structure to give the article a spinal cord. Forich (talk) 19:38, 29 November 2021 (UTC)
I propose the following structure:
- Drugs
- Antiviral drugs (drugs which attack the virus, including monoclonal antibodies)
- Other drugs
- Other treaments
In each section, the order is like this:
- Drugs approved by FDA (or EMA)
- Drugs which were approved by FDA (or EMA) but later the approval was revoked, or they lost their efficacy
- Drugs approved in some first-world countries, like Japan
- Drugs which were proposed but found not effective
- Experimental drugs
- All others
--Urod (talk) 17:57, 23 December 2021 (UTC)
- Great suggestion. We already have a "Medications" section which is equivalent to your "Drugs" proposal. Next step is, I think, to divide the "Medicaments" section into Antiviral and others. Forich (talk) 22:46, 15 October 2022 (UTC)
Nasal spray; something to maybe keep an eye out.
[edit]This is merely a nudge to have eyes follow a new proposed treatment. As of right now it doesn't satisfy WP:MEDRS.
There appears to be a nasal spray in development that has shown that it may be effective in preventing viral replication in some of the variants like Alpha and Beta. The manuscript hasn't gone through editing yet, but it can be viewed for the time being.[1]
—Tenryuu 🐲 ( 💬 • 📝 ) 02:12, 30 March 2022 (UTC)
Efficacy of early treatments
[edit]Currently, the article states that "Despite ongoing research, there is still not enough high-quality evidence to recommend so-called early treatment", with citations that are about a year old. Does anyone know if this situation has changed? It seems that there is at least one source (I do not know how reliable it is), which claims that there is scientific consensus building around the potential effectiveness of various things, e.g. Melatonin, Quercetin, and Curcumin. — Preceding unsigned comment added by Konne88 (talk • contribs) 20:00, 3 April 2022 (UTC)
TCM Herbal formulas against COVID-19
[edit]There has been done research by the Chinese concerning the development of new Traditional Chinese Medicine formulas against covid-19. It should be added in the main post. 2A02:AA12:E244:1080:9C91:5D6A:BA6E:3320 (talk) 11:04, 20 August 2022 (UTC)
Sources: L Jackal (talk) 11:17, 20 August 2022 (UTC)
I have sent a reply with a few sources on the matter but for some reason my comment is nowhere to be seen... L Jackal (talk) 11:21, 20 August 2022 (UTC)
New antibody treatments better than vaccines?
[edit]Of possible interest re Covid Treatment (9/8/2022) - several WP:RS[1][2] suggest that new antibody treatments may be better than vaccines - and worth considering (if not already of course) for the main article(s) - in any case - Stay Safe and Healthy !! - Drbogdan (talk) 17:05, 8 September 2022 (UTC)
References
- ^ Staff (8 September 2022). "Scientific Breakthrough Against COVID-19: Antibodies Identified That May Make Coronavirus Vaccines Unnecessary". Tel Aviv University. Retrieved 8 September 2022.
- ^ Li, Ruofan; et al. (5 August 2022). "Conformational flexibility in neutralization of SARS-CoV-2 by naturally elicited anti-SARS-CoV-2 antibodies". Communications Biology. 5: 789. doi:10.1038/s42003-022-03739-5. Retrieved 8 September 2022.
Drbogdan (talk) 17:05, 8 September 2022 (UTC)
First paragraph of lead is improvable
[edit]The first paragraph contains information that is outdated (april 2022), it does not summarizes the body of th article, it disregards the distinction of treatment in the early and late phases, and it lacks context overall.Forich (talk) 23:04, 15 October 2022 (UTC)
needs update
[edit]This article seems way, way out of date. Most of the dates are no later than 2022. OsamaBinLogin (talk) 15:26, 10 October 2024 (UTC)
- C-Class COVID-19 articles
- High-importance COVID-19 articles
- WikiProject COVID-19 articles
- C-Class Disaster management articles
- Low-importance Disaster management articles
- C-Class medicine articles
- Mid-importance medicine articles
- All WikiProject Medicine pages
- C-Class virus articles
- Mid-importance virus articles
- WikiProject Viruses articles