
Wellens' syndrome
| Wellens' syndrome | |
|---|---|
| Other names | Wellens' sign, Wellens' warning, Wellens' waves |
 | |
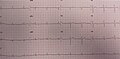
| EKG of a 69-year-old black male with Wellens' syndrome. Visible in leads V1-V4, here with a biphasic T-wave with negativisation. | |
| Specialty | Cardiology |
Wellens' syndrome is an electrocardiographic manifestation of critical proximal left anterior descending (LAD) coronary artery stenosis in people with unstable angina. Originally thought of as two separate types, A and B, it is now considered an evolving wave form, initially of biphasic T wave inversions and later becoming symmetrical, often deep (>2 mm), T wave inversions in the anterior precordial leads.[1]
First described by Hein J. J. Wellens and colleagues in 1982 in a subgroup of people with unstable angina,[2] it does not seem to be rare, appearing in 18% of patients in his original study. A subsequent prospective study identified this syndrome in 14% of patients at presentation and 60% of patients within the first 24 hours.[3]
The presence of Wellens' syndrome carries significant diagnostic and prognostic value. All people in the De Zwann's study with characteristic findings had more than 50% stenosis of the left anterior descending artery (mean = 85% stenosis) with complete or near-complete occlusion in 59%. In the original Wellens' study group, 75% of those with the typical syndrome manifestations had an anterior myocardial infarction. Sensitivity and specificity for significant (more or equal to 70%) stenosis of the LAD artery was found to be 69% and 89%, respectively, with a positive predictive value of 86%.[4]
Wellens' sign has also been seen as a rare presentation of Takotsubo cardiomyopathy or stress cardiomyopathy.[citation needed]
Diagnosis
[edit]The diagnosis is done via:[citation needed]
- Progressive symmetrical deep T wave inversion in leads V2 and V3
- Slope of inverted T waves generally at 60°-90°
- Little or no cardiac marker elevation
- Discrete or no ST segment elevation
- No loss of precordial R waves.
-
 Coronary angiogram, with video on the left showing tight, critical (95%) stenosis of the proximal LAD in a patient who had Wellens' warning; video on the right shows the same patient after reperfusion.
Coronary angiogram, with video on the left showing tight, critical (95%) stenosis of the proximal LAD in a patient who had Wellens' warning; video on the right shows the same patient after reperfusion. -
 EKG/ECG in someone with Wellens' syndrome when having chest pain
EKG/ECG in someone with Wellens' syndrome when having chest pain -
 EKG/ECG of the same person when pain-free, note the biphasic T waves in leads V2 and V3
EKG/ECG of the same person when pain-free, note the biphasic T waves in leads V2 and V3



References
[edit]- ^ Tandy, TK; Bottomy DP; Lewis JG (March 1999). "Wellens' syndrome". Annals of Emergency Medicine. 33 (3): 347–351. doi:10.1016/S0196-0644(99)70373-2. PMID 10036351.
- ^ de Zwaan, C; Bär FW; Wellens HJJ (April 1982). "Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction". American Heart Journal. 103 (4): 730–736. doi:10.1016/0002-8703(82)90480-X. PMID 6121481.
- ^ de Zwaan, C; Bär FW; Janssen JH; et al. (March 1989). "Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery". American Heart Journal. 117 (3): 657–665. doi:10.1016/0002-8703(89)90742-4. PMID 2784024.
- ^ Haines, DE; Raabe DS; Gundel WD; Wackers FJ (July 1983). "Anatomic and prognostic significance of new T-wave inversion in unstable angina". American Journal of Cardiology. 52 (1): 14–18. doi:10.1016/0002-9149(83)90061-9. PMID 6602539.